

Characteristics, drug combinations and dosages of primary care patients with uncontrolled ambulatory blood pressure and high medication adherence
- PMID: 23890931
- PMCID: PMC3883386
- DOI: 10.1016/j.jash.2013.06.004
Characteristics, drug combinations and dosages of primary care patients with uncontrolled ambulatory blood pressure and high medication adherence
Abstract
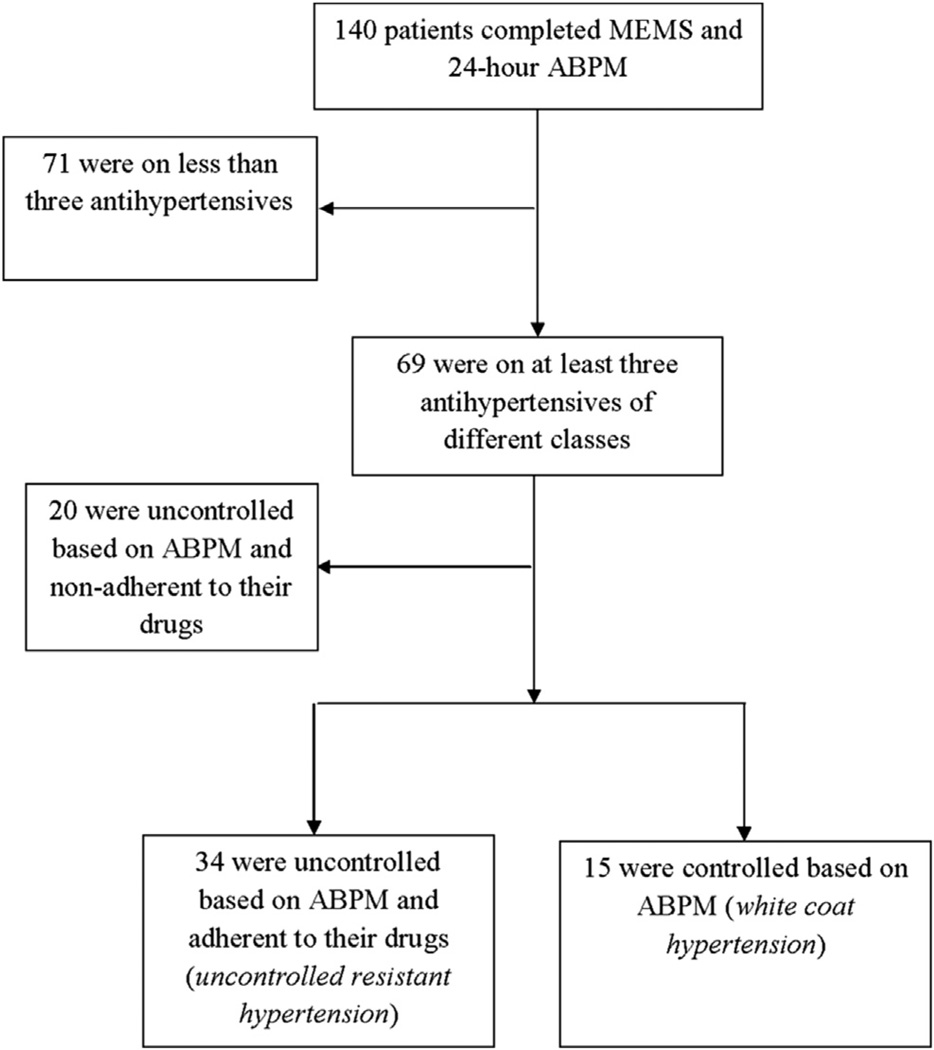
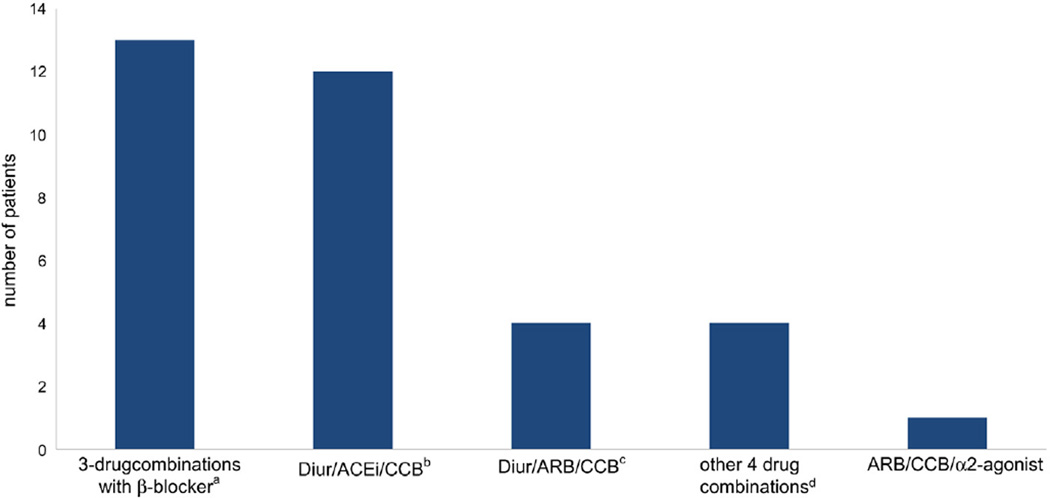
Most studies on the prevalence and determinants of resistant hypertension (RH) do not account for white coat hypertension, medication non-adherence, or use of suboptimal treatment dosages. We studied the characteristics, drug combinations, and dosages of patients on at least three antihypertensives of different classes who had uncontrolled blood pressure on 24-hour ambulatory blood pressure monitoring and high medication adherence measured by electronic monitoring. The data were collected as part of the baseline measures of a hypertension control trial. Of 140 monitored primary care patients, all with uncontrolled office blood pressure, 69 (49%) were on at least three antihypertensives of different classes. Of these 69, 15 (22%) were controlled on ambulatory blood pressure monitoring, 20 (29%) were uncontrolled and non-adherent, leaving only 34 (49%) adherent to their medications and having uncontrolled ambulatory hypertension (uncontrolled RH). Thirty-one (91%) of the 34 uncontrolled RH patients were prescribed a diuretic, of which 24 were on hydrochlorothiazide 25 mg. Less than half of the patients on angiotensin-converting enzyme inhibitor, angiotensin receptor blocker, or calcium channel blocker were prescribed maximal doses of these agents. Half of the RH can be attributed to white coat effect and poor medication adherence, and all of the remaining patients were on apparently suboptimal drug combinations and/or dosages. Primary care physicians need to be educated regarding the optimal treatment of RH.
Keywords: Resistant hypertension; drug dosage; electronic monitoring; medication adherence; white-coat hypertension.
Copyright © 2013 American Society of Hypertension. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
No conflict of interests to declare.
Figures
Comment in
-
Apparent and true resistant hypertension: why not the same?J Am Soc Hypertens. 2013 Nov-Dec;7(6):509-11. doi: 10.1016/j.jash.2013.07.007. Epub 2013 Sep 12. J Am Soc Hypertens. 2013. PMID: 24035315 No abstract available.
References
-
- Calhoun DA, Jones D, Textor S, Goff DC, Murphy TP, Toto RD, et al. Resistant hypertension: diagnosis, evaluation, and treatment: a scientific statement from the American Heart Association Professional Education Committee of the Council for High Blood Pressure Research. Circulation. 2008;117:e510–e526. - PubMed
-
- Cuspidi C, Macca G, Sampieri L, Michev I, Salerno M, Fusi V, et al. High prevalence of cardiac and extracardiac target organ damage in refractory hypertension. Journal Hypertens. 2001;19:2063–2070. - PubMed
-
- Persell SD. Prevalence of resistant hypertension in the United States, 2003–2008. Hypertension. 2011;57:1076–1080. - PubMed
-
- de la Sierra A, Segura J, Banegas JR, Gorostidi M, de la Cruz JJ, Armario P, et al. Clinical features of 8295 patients with resistant hypertension classified on the basis of ambulatory blood pressure monitoring. Hypertension. 2011;57:898–902. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
