

Predictors of outcome in acute encephalitis
- PMID: 23892708
- PMCID: PMC3908458
- DOI: 10.1212/WNL.0b013e3182a2cc6d
Predictors of outcome in acute encephalitis
Abstract
Objective: To investigate predictors of outcome in patients with all-cause encephalitis receiving care in the intensive care unit.
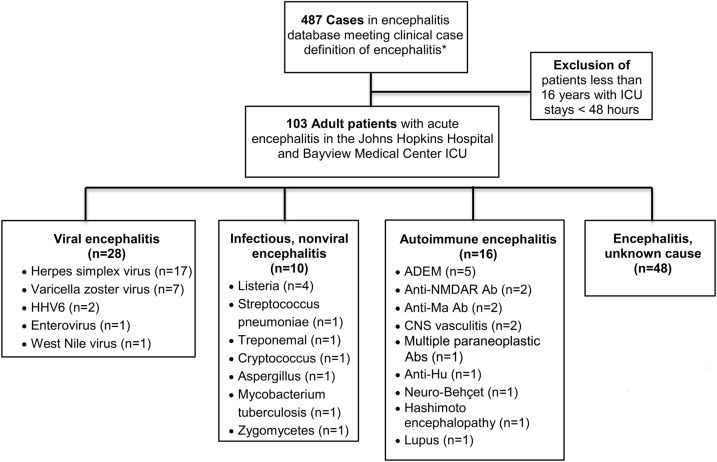
Methods: A retrospective analysis of encephalitis cases at The Johns Hopkins Hospital and Johns Hopkins Bayview Medical Center was performed. Using multivariate logistic regression analysis, we examined mortality and predictors of good outcome (defined as modified Rankin Scale scores of 1-3) and poor outcome (scores 4 and 5) in those surviving to hospital discharge.
Results: In our cohort of 103 patients, the median age was 52 years (interquartile range 26), 52 patients (50.49%) were male, 28 patients (27.18%) had viral encephalitis, 19 (18.45%) developed status epilepticus (SE), 15 (14.56%) had cerebral edema, and 19 (18.45%) died. In our multivariate logistic regression analysis, death was associated with cerebral edema (odds ratio [OR] 18.06, 95% confidence interval [CI] 3.14-103.92), SE (OR 8.16, 95% CI 1.55-43.10), and thrombocytopenia (OR 6.28, 95% CI 1.41-28.03). Endotracheal intubation requirement with ventilator support was highly correlated with death (95%). In addition, in those patients who survived, viral, nonviral, and unknown causes of encephalitis were less likely to have a poor outcome at hospital discharge compared with an autoimmune etiology (viral encephalitis: OR 0.09, 95% CI 0.01-0.57; nonviral encephalitis: OR 0.02, 95% CI 0.01-0.31; unknown etiology: OR 0.18, 95% CI 0.04-0.91).
Conclusions: Our study suggests that predictors of death in patients with encephalitis comprise potentially reversible conditions including cerebral edema, SE, and thrombocytopenia. Further prospective studies are needed to determine whether aggressive management of these complications in patients with encephalitis improves outcome.
Figures
References
-
- Glaser CA, Gilliam S, Schnurr D, et al. In search of encephalitis etiologies: diagnostic challenges in the California Encephalitis Project, 1998–2000. Clin Infect Dis 2003;36:731–742 - PubMed
-
- Whitley RJ, Lakeman F. Herpes simplex virus infections of the central nervous system: therapeutic and diagnostic considerations. Clin Infect Dis 1995;20:414–420 - PubMed
-
- Granerod J, Tam CC, Crowcroft NS, Davies NW, Borchert M, Thomas SL. Challenge of the unknown: a systematic review of acute encephalitis in non-outbreak situations. Neurology 2010;75:924–932 - PubMed
-
- Steiner I, Budka H, Chaudhuri A, et al. Viral meningoencephalitis: a review of diagnostic methods and guidelines for management. Eur J Neurol 2010;17:999–e57 - PubMed
-
- Tunkel AR, Glaser CA, Bloch KC, et al. The management of encephalitis: clinical practice guidelines by the Infectious Diseases Society of America. Clin Infect Dis 2008;47:303–327 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical