

Sonographic predictors of postnatal bowel atresia in fetal gastroschisis
- PMID: 23893619
- PMCID: PMC3968234
- DOI: 10.1002/uog.12568
Sonographic predictors of postnatal bowel atresia in fetal gastroschisis
Abstract
Objectives: To estimate the association between antenatal bowel dilation and postnatal small-bowel atresia in fetal gastroschisis and to establish a threshold at which the risk of adverse neonatal outcome increases.
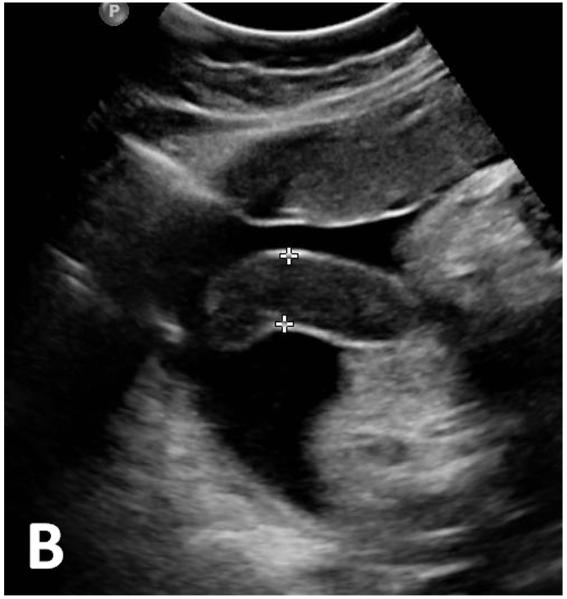
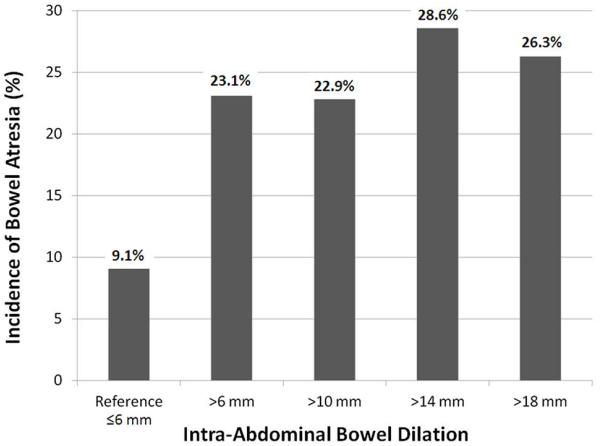
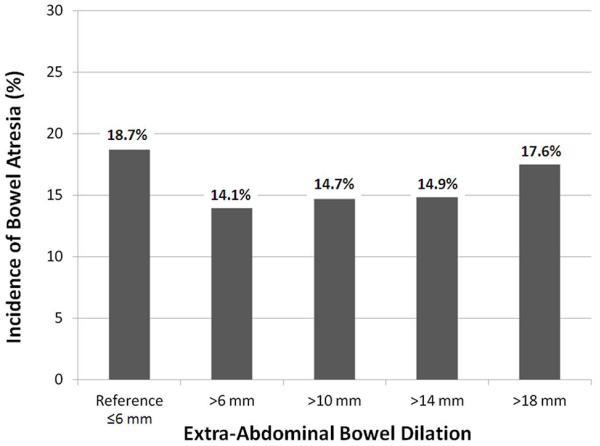
Methods: This was a retrospective cohort study of singleton gestations with an antenatal diagnosis of gastroschisis seen in our ultrasound unit from 2001 to 2010. We reviewed stored images from the last ultrasound examination before delivery, blinded to postnatal diagnoses and outcomes. Fetal intra- and extra-abdominal bowel dilation (IABD and EABD, respectively) and bowel-wall thickness were measured. Previously published definitions of bowel dilation, including > 6, > 10, > 14 and > 18 mm, were evaluated for association with the primary outcome of bowel atresia. The optimal threshold to define fetal bowel dilation was determined by evaluating the significance of association as well as test performance characteristics.
Results: Of 109 consecutive patients with fetal gastroschisis, there were four cases of intrauterine fetal demise and three neonatal deaths. Of the 94 live births with complete outcome data, 39 (41.5%) had measurable IABD. There were 14 (14.9%) cases of bowel atresia. Using a threshold of > 14 mm, IABD was significantly associated with an increased risk for bowel atresia (relative risk, 3.1 (95% CI, 1.2-8.2)) with a sensitivity of 57.1%, specificity of 75.0%, positive predictive value of 28.6% and negative predictive value of 90.9%. IABD > 14 mm was also associated with a significantly longer stay in neonatal intensive care unit. There was no significant association between EABD and bowel atresia at any of the thresholds evaluated.
Conclusion: IABD > 14 mm is associated with an increased risk for postnatal bowel atresia in fetal gastroschisis. This finding may be useful in counseling patients regarding the anticipated postnatal course for their neonate.
Keywords: abdominal wall defect; bowel atresia; bowel dilation; bowel-wall thickening; gastroschisis.
Copyright © 2013 ISUOG. Published by John Wiley & Sons Ltd.
Figures


References
-
- Fillingham A, Rankin J. Prevalence, prenatal diagnosis and survival of gastroschisis. Prenat Diagn. 2008;13:1232–1237. - PubMed
-
- Wilson RD, Johnson MP. Congenital abdominal wall defects: an update. Fetal Diagn Ther. 2004;19:385–398. - PubMed
-
- Molik KA, Gingalewski CA, West KW, Rescorla FJ, Scherer LR, Engum SA, Grosfeld JL. Gastroschisis: a plea for risk categorization. J Pediatri Surg. 2001;36:51–55. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
