

Niclosamide overcomes acquired resistance to erlotinib through suppression of STAT3 in non-small cell lung cancer
- PMID: 23894143
- PMCID: PMC3795834
- DOI: 10.1158/1535-7163.MCT-13-0095
Niclosamide overcomes acquired resistance to erlotinib through suppression of STAT3 in non-small cell lung cancer
Abstract
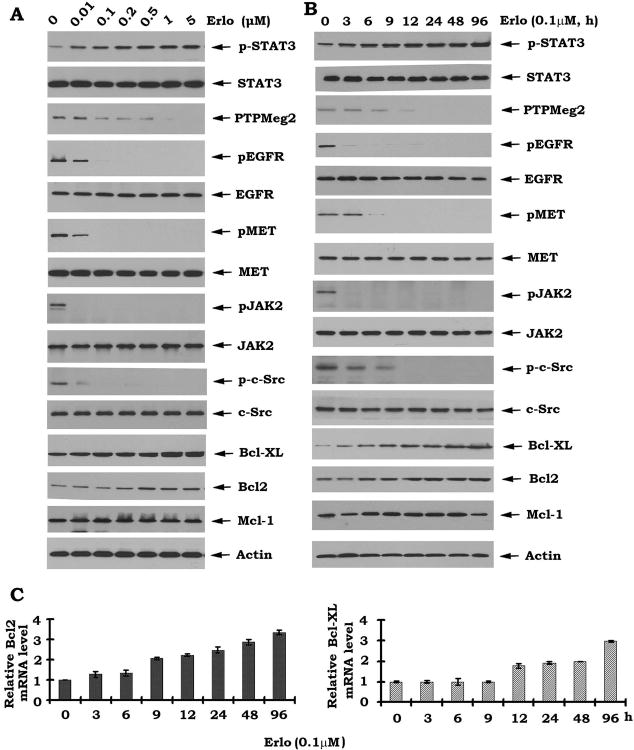
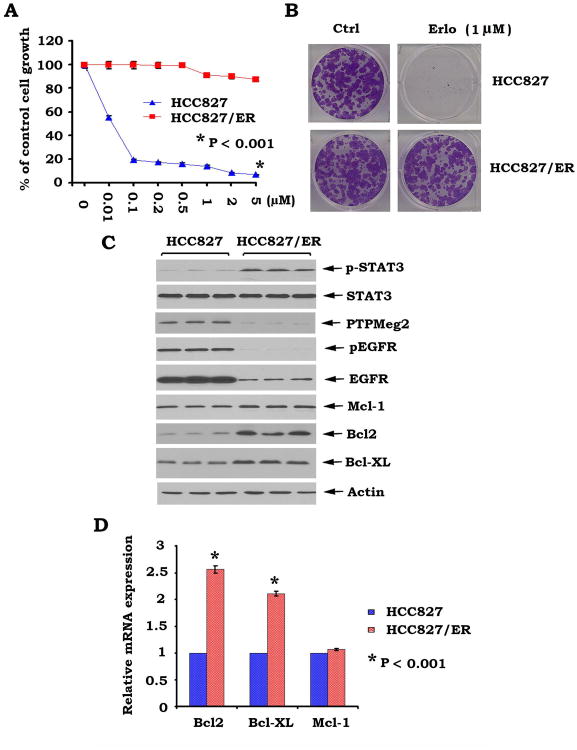
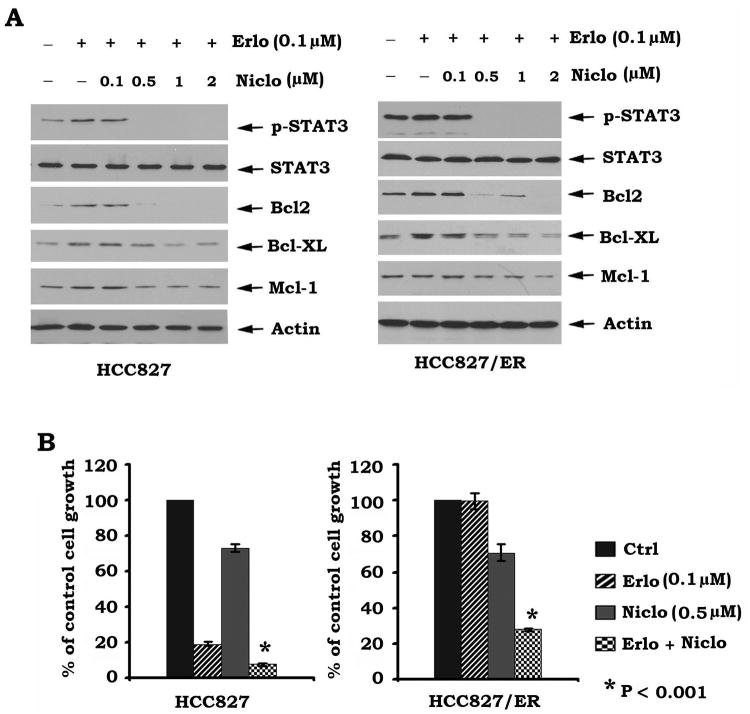
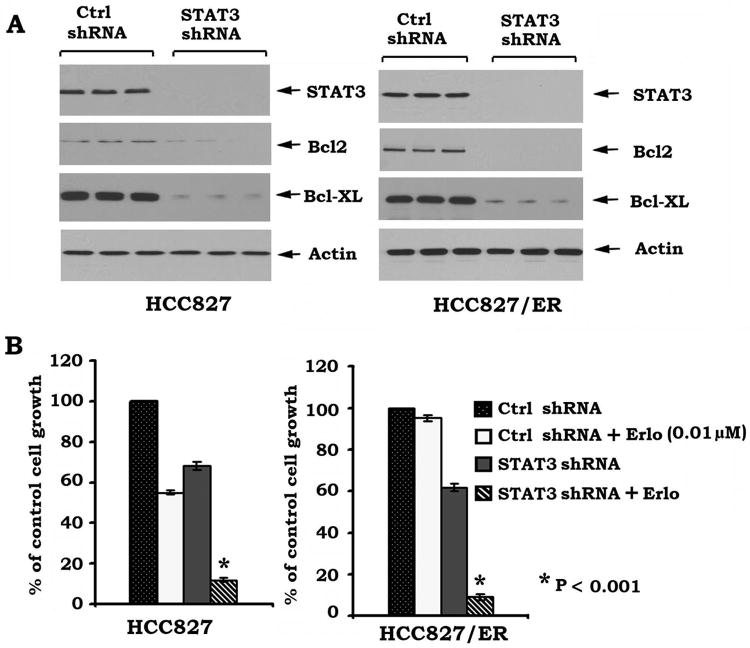
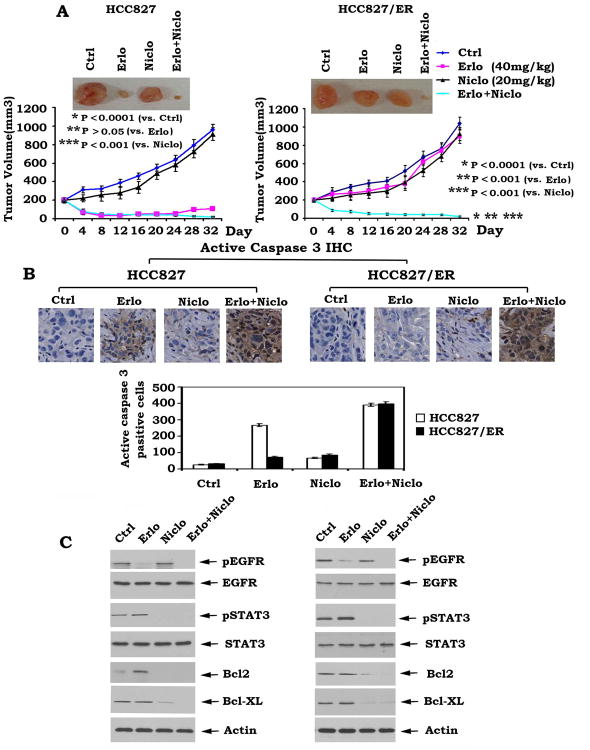
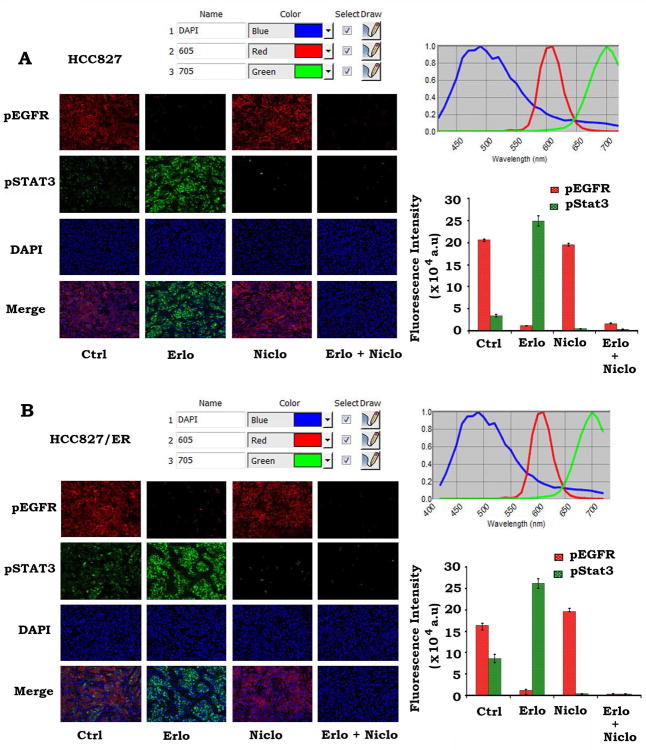
The emergence of resistance to EGF receptor (EGFR) inhibitor therapy is a major clinical problem for patients with non-small cell lung cancer (NSCLC). The mechanisms underlying tumor resistance to inhibitors of the kinase activity of EGFR are not fully understood. Here, we found that inhibition of EGFR by erlotinib induces STAT3 phosphorylation at Tyr705 in association with increased Bcl2/Bcl-XL at both mRNA and protein levels in various human lung cancer cells. PTPMeg2 is a physiologic STAT3 phosphatase that can directly dephosphorylate STAT3 at the Tyr705 site. Intriguingly, treatment of cells with erlotinib results in downregulation of PTPMeg2 without activation of STAT3 kinases [i.e., Janus-activated kinase (JAK2) or c-Src], suggesting that erlotinib-enhanced phosphorylation of STAT3 may occur, at least in part, from suppression of PTPMeg2 expression. Because elevated levels of phosphorylated STAT3 (pSTAT3), Bcl2, and Bcl-XL were observed in erlotinib-resistant lung cancer (HCC827/ER) cells as compared with erlotinib-sensitive parental HCC827 cells, we postulate that the erlotinib-activated STAT3/Bcl2/Bcl-XL survival pathway may contribute to acquired resistance to erlotinib. Both blockage of Tyr705 phosphorylation of STAT3 by niclosamide and depletion of STAT3 by RNA interference in HCC827/ER cells reverse erlotinib resistance. Niclosamide in combination with erlotinib potently represses erlotinib-resistant lung cancer xenografts in association with increased apoptosis in tumor tissues, suggesting that niclosamide can restore sensitivity to erlotinib. These findings uncover a novel mechanism of erlotinib resistance and provide a novel approach to overcome resistance by blocking the STAT3/Bcl2/Bcl-XL survival signaling pathway in human lung cancer.
©2013 AACR.
Conflict of interest statement
Figures

References
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin. 2012;62:10–29. - PubMed
-
- Jemal A, Siegel R, Ward E, Murray T, Xu J, Thun MJ. Cancer statistics, 2007. CA Cancer J Clin. 2007;57:43–66. - PubMed
-
- da Cunha Santos G, Shepherd FA, Tsao MS. EGFR mutations and lung cancer. Annu Rev Pathol. 2011;6:49–69. - PubMed
-
- Gridelli C, Maione P, Bareschino MA, Schettino C, Sacco PC, Ambrosio R, et al. Erlotinib in the treatment of non-small cell lung cancer: current status and future developments. Anticancer Res. 2010;30:1301–10. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
Miscellaneous
