

Improving antibiotic prescribing in acute respiratory tract infections: cluster randomised trial from Norwegian general practice (prescription peer academic detailing (Rx-PAD) study)
- PMID: 23894178
- PMCID: PMC3724398
- DOI: 10.1136/bmj.f4403
Improving antibiotic prescribing in acute respiratory tract infections: cluster randomised trial from Norwegian general practice (prescription peer academic detailing (Rx-PAD) study)
Abstract
Objective: To assess the effects of a multifaceted educational intervention in Norwegian general practice aiming to reduce antibiotic prescription rates for acute respiratory tract infections and to reduce the use of broad spectrum antibiotics.
Design: Cluster randomised controlled study.
Setting: Existing continuing medical education groups were recruited and randomised to intervention or control.
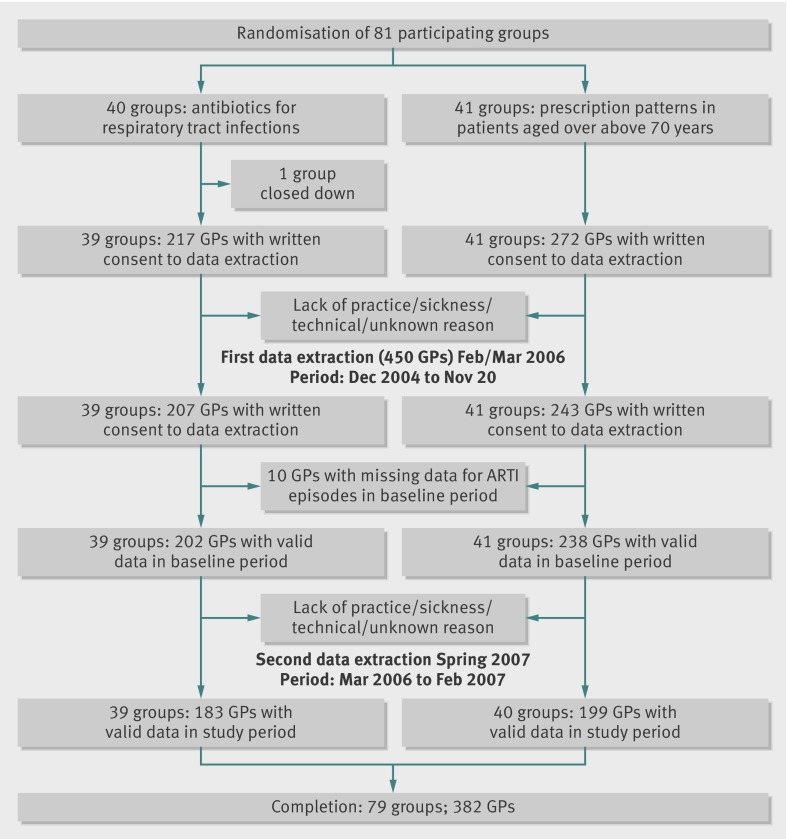
Participants: 79 groups, comprising 382 general practitioners, completed the interventions and data extractions.
Interventions: The intervention groups had two visits by peer academic detailers, the first presenting the national clinical guidelines for antibiotic use and recent research evidence on acute respiratory tract infections, the second based on feedback reports on each general practitioner's antibiotic prescribing profile from the preceding year. Regional one day seminars were arranged as a supplement. The control arm received a different intervention targeting prescribing practice for older patients.
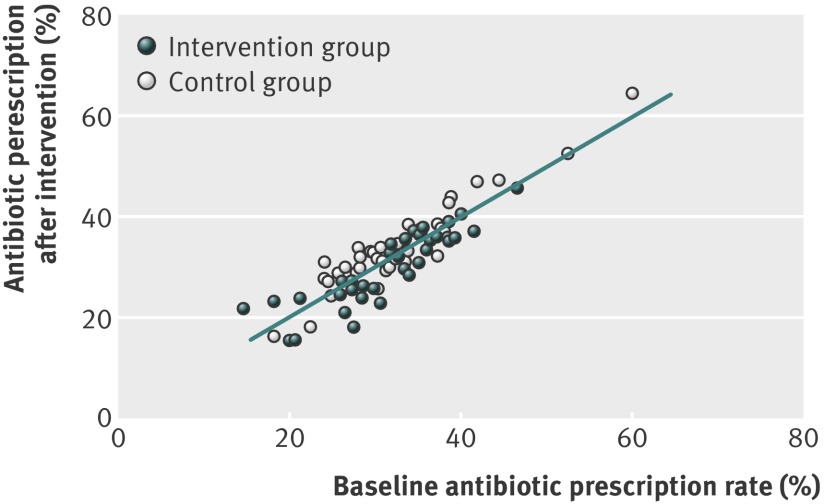
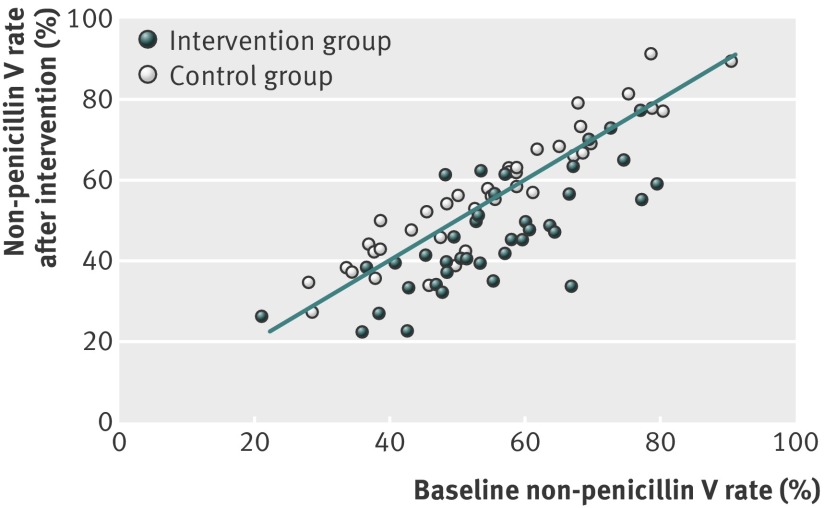
Main outcome measures: Prescription rates and proportion of non-penicillin V antibiotics prescribed at the group level before and after the intervention, compared with corresponding data from the controls.
Results: In an adjusted, multilevel model, the effect of the intervention on the 39 intervention groups (183 general practitioners) was a reduction (odds ratio 0.72, 95% confidence interval 0.61 to 0.84) in prescribing of antibiotics for acute respiratory tract infections compared with the controls (40 continuing medical education groups with 199 general practitioners). A corresponding reduction was seen in the odds (0.64, 0.49 to 0.82) for prescribing a non-penicillin V antibiotic when an antibiotic was issued. Prescriptions per 1000 listed patients increased from 80.3 to 84.6 in the intervention arm and from 80.9 to 89.0 in the control arm, but this reflects a greater incidence of infections (particularly pneumonia) that needed treating in the intervention arm.
Conclusions: The intervention led to improved antibiotic prescribing for respiratory tract infections in a representative sample of Norwegian general practitioners, and the courses were feasible to the general practitioners.
Trial registration: Clinical trials NCT00272155.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
References
-
- Goossens H, Ferech M, Vander SR, Elseviers M. Outpatient antibiotic use in Europe and association with resistance: a cross-national database study. Lancet 2005;365:579-87. - PubMed
-
- Seppala H, Klaukka T, Vuopio-Varkila J, Muotiala A, Helenius H, Lager K, et al. The effect of changes in the consumption of macrolide antibiotics on erythromycin resistance in group A streptococci in Finland. N Engl J Med 1997;337:441-6. - PubMed
-
- Costelloe C, Metcalfe C, Lovering A, Mant D, Hay AD. Effect of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: systematic review and meta-analysis. BMJ 2010;340:c2096. - PubMed
-
- NORM/NORM-VET 2010. Usage of antimicrobial agents and occurrence of antimicrobial resistance in Norway. Norwegian Surveillance System for Antimicrobial Drug Resistance, 2011:1502-2307.
-
- Guidelines to antibiotic treatment in general practice [Antibiotikabehandling i allmennpraksis]. Norwegian Board of Health, 2000.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical