

A gene signature to determine metastatic behavior in thymomas
- PMID: 23894276
- PMCID: PMC3722217
- DOI: 10.1371/journal.pone.0066047
A gene signature to determine metastatic behavior in thymomas
Abstract
Purpose: Thymoma represents one of the rarest of all malignancies. Stage and completeness of resection have been used to ascertain postoperative therapeutic strategies albeit with limited prognostic accuracy. A molecular classifier would be useful to improve the assessment of metastatic behaviour and optimize patient management.
Methods: qRT-PCR assay for 23 genes (19 test and four reference genes) was performed on multi-institutional archival primary thymomas (n = 36). Gene expression levels were used to compute a signature, classifying tumors into classes 1 and 2, corresponding to low or high likelihood for metastases. The signature was validated in an independent multi-institutional cohort of patients (n = 75).
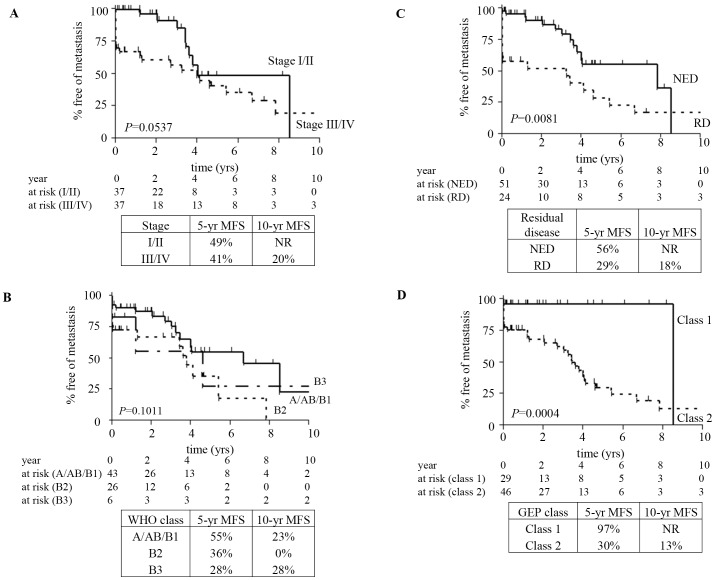
Results: A nine-gene signature that can predict metastatic behavior of thymomas was developed and validated. Using radial basis machine modeling in the training set, 5-year and 10-year metastasis-free survival rates were 77% and 26% for predicted low (class 1) and high (class 2) risk of metastasis (P = 0.0047, log-rank), respectively. For the validation set, 5-year metastasis-free survival rates were 97% and 30% for predicted low- and high-risk patients (P = 0.0004, log-rank), respectively. The 5-year metastasis-free survival rates for the validation set were 49% and 41% for Masaoka stages I/II and III/IV (P = 0.0537, log-rank), respectively. In univariate and multivariate Cox models evaluating common prognostic factors for thymoma metastasis, the nine-gene signature was the only independent indicator of metastases (P = 0.036).
Conclusion: A nine-gene signature was established and validated which predicts the likelihood of metastasis more accurately than traditional staging. This further underscores the biologic determinants of the clinical course of thymoma and may improve patient management.
Conflict of interest statement
Figures

References
-
- Engels EA, Pfeiffer RM (2003) Malignant thymoma in the United States: demographic patterns in incidence and associations with subsequent malignancies. Int J Cancer 105: 546–551. - PubMed
-
- Okumura M, Ohta M, Tateyama H, Nakagawa K, Matsumura A, et al. (2002) The World Health Organization histologic classification system reflects the oncologic behavior of thymoma: a clinical study of 273 patients. Cancer 94: 624–632. - PubMed
-
- Okumura M, Miyoshi S, Fujii Y, Takeuchi Y, Shiono H, et al. (2001) Clinical and functional significance of WHO classification on human thymic epithelial neoplasms: a study of 146 consecutive tumors. Am J Surg Pathol 25: 103–110. - PubMed
-
- Moran CA, Suster S (2008) The World Health Organization (WHO) histologic classification of thymomas: a reanalysis. Curr Treat Options Oncol 9: 288–299. - PubMed
-
- Jain RK, Mehta RJ, Henley JD, Kesler KA, Loehrer PJ, et al. (2010) WHO types A and AB thymomas: not always benign. Mod Pathol 23: 1641–1649. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
