

Recovery of adrenal function after long-term glucocorticoid therapy for giant cell arteritis: a cohort study
- PMID: 23894335
- PMCID: PMC3722149
- DOI: 10.1371/journal.pone.0068713
Recovery of adrenal function after long-term glucocorticoid therapy for giant cell arteritis: a cohort study
Abstract
Objectives: Giant cell arteritis (GCA) is a chronic systemic vasculitis of large and medium-sized arteries, for which long-term glucocorticoid (GC) treatment is needed. During GC withdrawal patients can suffer adrenal insufficiency. We sought to determine the time until recovery of adrenal function after long-term GC therapy, and to assess the prevalence and predictors for secondary adrenal insufficiency.
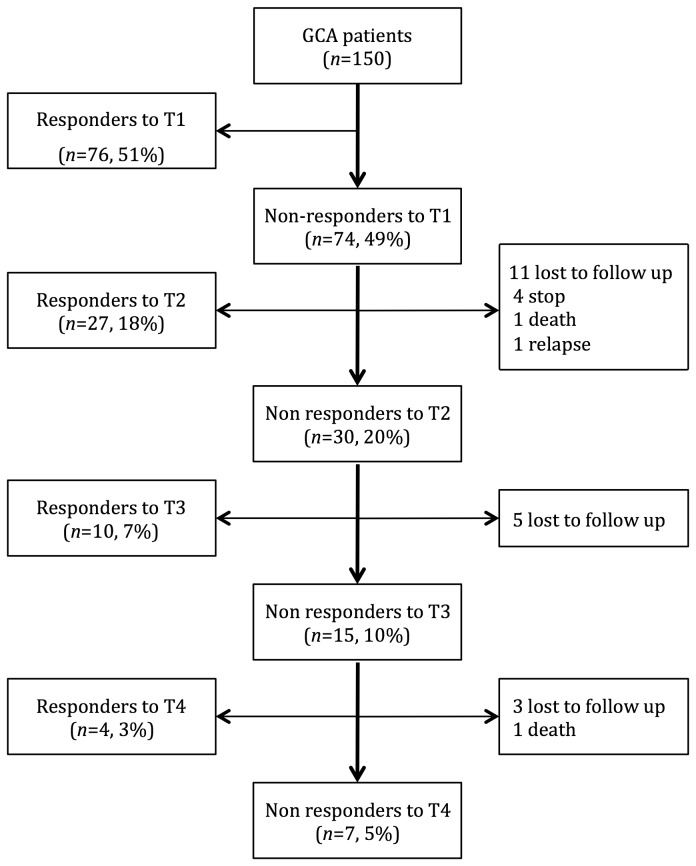
Subjects and design: 150 patients meeting the ACR criteria for GCA between 1984 and 2012 were analyzed. All received the same GC treatment protocol. The low-dose ACTH stimulation test was repeated annually until adrenal recovery. Biographical, clinical and laboratory data were collected prospectively and compared.
Results: At the first ACTH test, 74 (49%) patients were non-responders: of these, the mean time until recovery of adrenal function was 14 months (max: 51 months). A normal test response occurred within 36 months in 85% of patients. However, adrenal function never recovered in 5% of patients. GC of >15 mg/day at 6 months, GC of >9.5 mg/day at 12 months, treatment duration of >19 months, a cumulative GC dose of >8.5 g, and a basal cortisol concentration of <386 nmol/L were all statistically associated with a negative response in the first ACTH test (p <0.05).
Conclusion: Adrenal insufficiency in patients with GCA, treated long-term with GC, was frequent but transitory. Thus, physicians' vigilance should be increased and an ACTH test should be performed when GC causes the above associated statistical factors.
Conflict of interest statement
Figures
References
-
- Borchers AT, Gershwin ME (2012) Giant cell arteritis: a review of classification, pathophysiology, geoepidemiology and treatment. Autoimmun Rev 11: A544-A554. doi:10.1016/j.autrev.2012.01.003. PubMed: 22285588. - DOI - PubMed
-
- Hunder GG, Sheps SG, Allen GL, Joyce JW. Daily and alternate-day corticosteroid regimens in treatment of giant cell arteritis: comparison in a prospective study. (1975) Ann Intern Med 82: 613-618. - PubMed
-
- Straub RH, Paimela L, Peltomaa R, Schölmerich J, Leirisalo-Repo M (2002) Inadequately low serum levels of steroid hormones in relation to interleukin-6 and tumor necrosis factor in untreated patients with early rheumatoid arthritis and reactive arthritis. Arthritis Rheum 46: 654-662. doi:10.1002/art.10177. PubMed: 11920401. - DOI - PubMed
-
- Bornstein SR (2009) Predisposing factors for adrenal insufficiency. N Engl J Med 360: 2328-2339. doi:10.1056/NEJMra0804635. PubMed: 19474430. - DOI - PubMed
-
- Lansang MC, Hustak LK (2011) Glucocorticoid-induced diabetes and adrenal suppression: how to detect and manage them. Cleve Clin J Med 78: 748-756. doi:10.3949/ccjm.78a.10180. PubMed: 22049542. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
