

Incidence and mortality of acute kidney injury after myocardial infarction: a comparison between KDIGO and RIFLE criteria
- PMID: 23894572
- PMCID: PMC3720921
- DOI: 10.1371/journal.pone.0069998
Incidence and mortality of acute kidney injury after myocardial infarction: a comparison between KDIGO and RIFLE criteria
Abstract
Background: Acute kidney injury (AKI) increases the risk of death after acute myocardial infarction (AMI). Recently, a new AKI definition was proposed by the Kidney Disease Improving Global Outcomes (KDIGO) organization. The aim of the current study was to compare the incidence and the early and late mortality of AKI diagnosed by RIFLE and KDIGO criteria in the first 7 days of hospitalization due to an AMI.
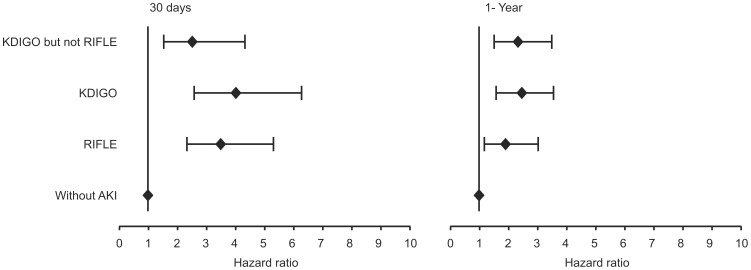
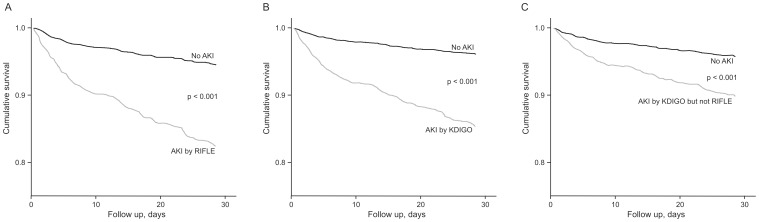
Methods and results: In total, 1,050 AMI patients were prospectively studied. AKI defined by RIFLE and KDIGO occurred in 14.8% and 36.6% of patients, respectively. By applying multivariate Cox analysis, AKI was associated with an increased adjusted hazard ratio (AHR) for 30-day death of 3.51 (95% confidence interval [CI] 2.35-5.25, p<0.001) by RIFLE and 3.99 (CI 2.59-6.15, p<0.001) by KDIGO and with an AHR for 1-year mortality of 1.84 (CI 1.12-3.01, p=0.016) by RIFLE and 2.43 (CI 1.62-3.62, p<0.001) by KDIGO. The subgroup of patients diagnosed as non-AKI by RIFLE but as AKI by KDIGO criteria had also an increased AHR for death of 2.55 (1.52-4.28) at 30 days and 2.28 (CI 1.46-3.54) at 1 year (p<0.001).
Conclusions: KDIGO criteria detected substantially more AKI patients than RIFLE among AMI patients. Patients diagnosed as AKI by KDIGO but not RIFLE criteria had a significantly higher early and late mortality. In this study KDIGO criteria were more suitable for AKI diagnosis in AMI patients than RIFLE criteria.
Conflict of interest statement
Figures


References
-
- Goldberg A, Hammerman H, Petcherski S, Zdorovyak A, Yalonetsky S, et al. (2005) Inhospital and 1-year mortality of patients who develop worsening renal function following acute ST-elevation myocardial infarction. Am Heart J 150: 330–337. - PubMed
-
- Newsome BB, Warnock DG, McClellan WM, Herzog CA, Kiefe CI, et al. (2008) Long-term risk of mortality and end-stage renal disease among the elderly after small increases in serum creatinine level during hospitalization for acute myocardial infarction. Arch Intern Med 168: 609–616. - PubMed
-
- Parikh CR, Coca SG, Wang Y, Masoudi FA, Krumholz HM (2008) Long-term prognosis of acute kidney injury after acute myocardial infarction. Arch Intern Med 168: 987–995. - PubMed
-
- Marenzi G, Assanelli E, Campodonico J, De Metrio M, Lauri G, et al. (2010) Acute kidney injury in ST-segment elevation acute myocardial infarction complicated by cardiogenic shock at admission. Crit Care Med 38: 438–444. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
