

Soluble isoform of the receptor for advanced glycation end products as a biomarker for postoperative respiratory failure after cardiac surgery
- PMID: 23894617
- PMCID: PMC3720894
- DOI: 10.1371/journal.pone.0070200
Soluble isoform of the receptor for advanced glycation end products as a biomarker for postoperative respiratory failure after cardiac surgery
Abstract
Purpose: Postoperative respiratory failure is a major problem which can prolong the stay in the intensive care unit in patients undergoing cardiac surgery. We measured the serum levels of the soluble isoform of the receptor for advanced glycation end products (sRAGE), and we studied its association with postoperative respiratory failure.
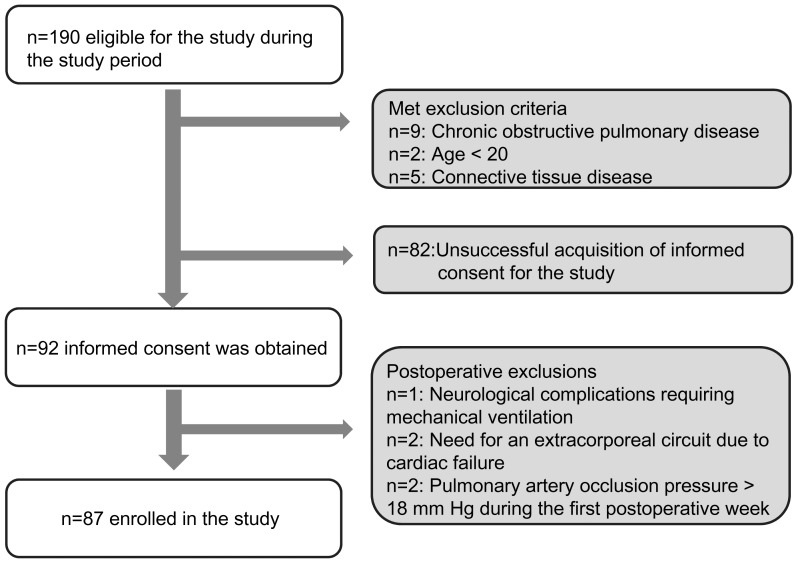
Methods: Eighty-seven patients undergoing elective cardiac surgery were enrolled in this multicenter observational study in three university hospitals. Serum biomarker levels were measured perioperatively, and clinical data were collected for 7 days postoperatively. The duration of mechanical ventilation was studied for 28 days.
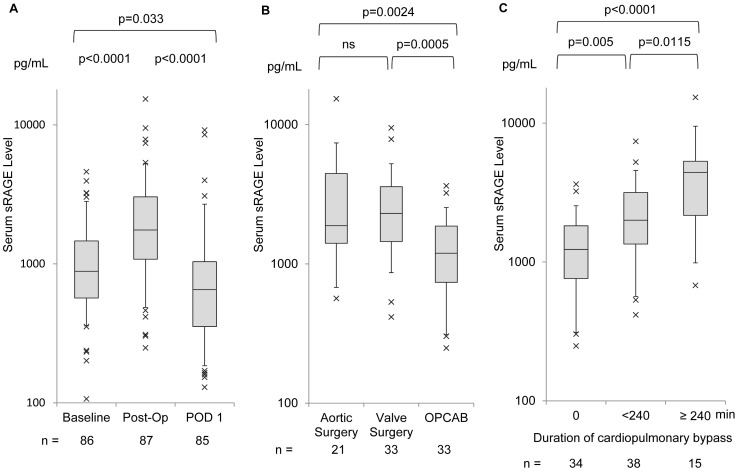
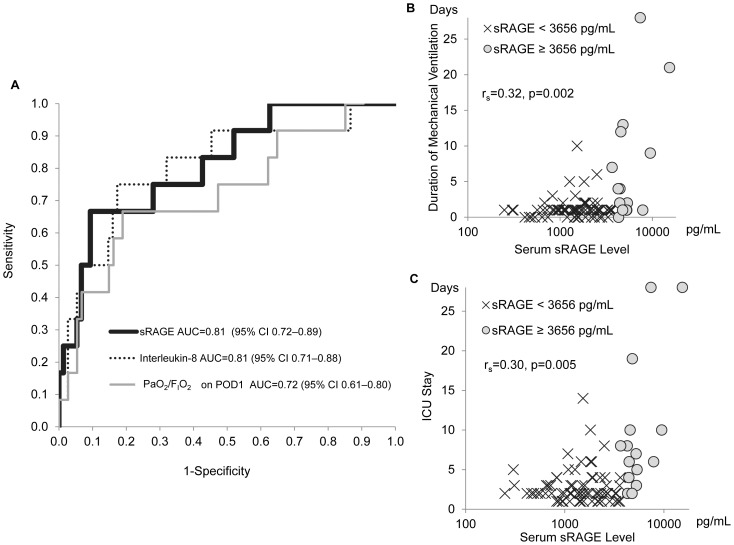
Results: Serum levels of sRAGE elevated immediately after surgery (median, 1751 pg/mL; interquartile range (IQR) 1080-3034 pg/mL) compared with the level after anesthetic induction (median, 884 pg/mL; IQR, 568-1462 pg/mL). Postoperative sRAGE levels in patients undergoing off-pump coronary artery bypass grafting (median, 1193 pg/mL; IQR 737-1869 pg/mL) were significantly lower than in patients undergoing aortic surgery (median, 1883 pg/mL; IQR, 1406-4456 pg/mL; p=0.0024) and valve surgery (median, 2302 pg/mL; IQR, 1447-3585 pg/mL; p=0.0005), and postoperative sRAGE correlated moderately with duration of cardiopulmonary bypass (rs =0.44, p<0.0001). Receiver operating characteristic curve analysis demonstrated that postoperative sRAGE had a predictive performance with area under the curve of 0.81 (95% confidence interval 0.71-0.88) for postoperative respiratory failure, defined as prolonged mechanical ventilation >3 days. The optimum cutoff value for prediction of respiratory failure was 3656 pg/mL, with sensitivity and specificity of 62% and 91%, respectively.
Conclusions: Serum sRAGE levels elevated immediately after cardiac surgery, and the range of elevation was associated with the morbidity of postoperative respiratory failure. Early postoperative sRAGE levels appear to be linked to cardiopulmonary bypass, and may have predictive performance for postoperative respiratory failure; however, large-scale validation studies are needed.
Conflict of interest statement
Figures
References
-
- Paparella D, Yau TM, Young E (2002) Cardiopulmonary bypass induced inflammation: pathophysiology and treatment. An update. Eur J Cardiothorac Surg 21: 232–244. - PubMed
-
- Ranieri VM, Vitale N, Grasso S, Puntillo F, Mascia L, et al. (1999) Time-course of impairment of respiratory mechanics after cardiac surgery and cardiopulmonary bypass. Crit Care Med 27: 1454–1460. - PubMed
-
- Filsoufi F, Rahmanian PB, Castillo JG, Chikwe J, Adams DH (2008) Predictors and early and late outcomes of respiratory failure in contemporary cardiac surgery. Chest 133: 713–721. - PubMed
-
- Reddy SL, Grayson AD, Griffiths EM, Pullan DM, Rashid A (2007) Logistic risk model for prolonged ventilation after adult cardiac surgery. Ann Thorac Surg 84: 528–536. - PubMed
-
- Pappalardo F, Franco A, Landoni G, Cardano P, Zangrillo A, et al. (2004) Long-term outcome and quality of life of patients requiring prolonged mechanical ventilation after cardiac surgery. Eur J Cardiothorac Surg 25: 548–552. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
