

Is adrenalectomy necessary during unilateral nephrectomy for Wilms Tumor? A report from the Children's Oncology Group
- PMID: 23895979
- PMCID: PMC5652039
- DOI: 10.1016/j.jpedsurg.2013.04.019
Is adrenalectomy necessary during unilateral nephrectomy for Wilms Tumor? A report from the Children's Oncology Group
Abstract
Purpose: To determine whether performing adrenalectomy at the time of nephrectomy for unilateral Wilms tumor impacts clinical outcome.
Methods: We reviewed information on all patients enrolled on National Wilms Tumor Study-4 and -5. Data were abstracted on patient demographics, tumor characteristics, surgical and pathologic status of the adrenal gland, and patient outcomes. The primary endpoints were intraoperative spill and five-year event-free survival (EFS) in patients who did or did not undergo adrenalectomy.
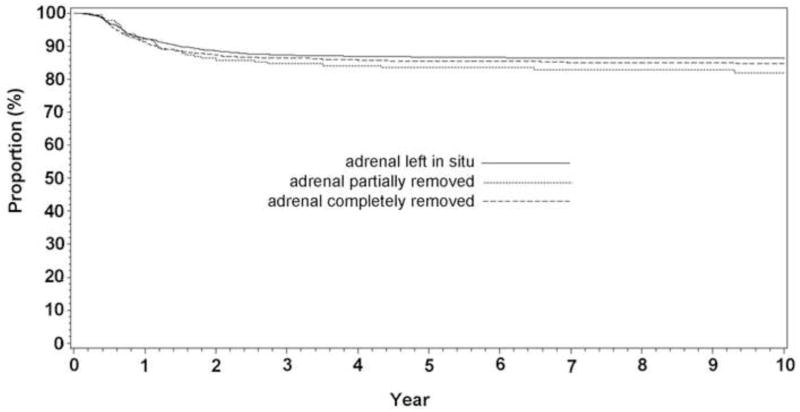
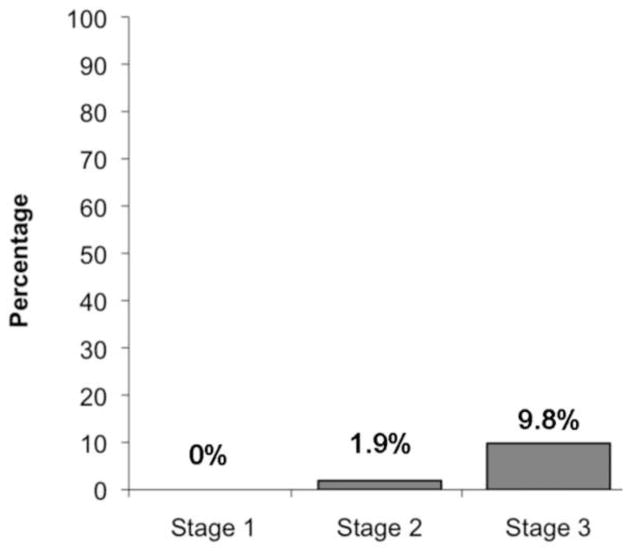
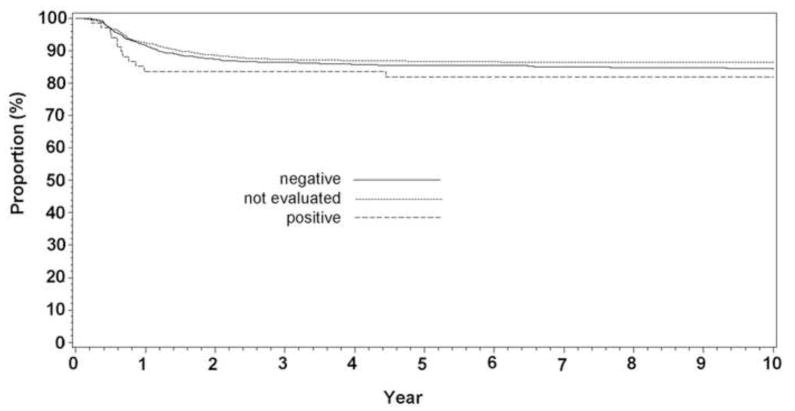
Results: Of 3825 patients with complete evaluable data, the adrenal was left in situ in 2264 (57.9%) patients, and was removed completely in 1367 patients (36.7%) or partially in 194 patients (5.2%). Of the adrenal glands removed, 68 (4.4%) contained tumor. Adrenal involvement was more common in patients with stage 3 (9.8%) than stage 2 disease (1.9%; p < 0.0001). After controlling for stage and histopathology, five-year EFS was similar whether or not the adrenal gland was removed (p = 0.48), or involved with tumor (p = 0.81); however, intraoperative spill rates were higher in patients undergoing adrenalectomy (26.1% vs 15.5%, p < 0.0001), likely due to larger tumor size or technical factors. No patient had clinical evidence of adrenal insufficiency or tumor recurrence in the adrenal gland during follow-up (median 9.9 years).
Conclusions: Sparing the adrenal gland during nephrectomy for unilateral Wilms tumor was not associated with a higher incidence of intraoperative spill and was associated with a similar oncologic outcome, on a per-stage basis, with cases where the adrenal was removed. Thus, adrenalectomy should not be considered mandatory during radical nephrectomy for Wilms tumor.
Keywords: Adrenalectomy; Pediatric renal tumor; Wilms tumor.
Copyright © 2013 Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Can we spare removing the adrenal gland at radical nephrectomy in children with wilms tumor?J Urol. 2010 Oct;184(4 Suppl):1638-43. doi: 10.1016/j.juro.2010.03.126. Epub 2010 Aug 21. J Urol. 2010. PMID: 20728101
-
Practice status and influencing factors of adrenalectomy in patients with Wilms tumor.Asian J Surg. 2023 Jan;46(1):52-57. doi: 10.1016/j.asjsur.2022.05.004. Epub 2022 May 23. Asian J Surg. 2023. PMID: 35618582 Review.
-
Clinical Outcome and Biological Predictors of Relapse After Nephrectomy Only for Very Low-risk Wilms Tumor: A Report From Children's Oncology Group AREN0532.Ann Surg. 2017 Apr;265(4):835-840. doi: 10.1097/SLA.0000000000001716. Ann Surg. 2017. PMID: 27811504 Free PMC article.
-
Ipsilateral adrenalectomy at the time of radical nephrectomy impacts overall survival.BJU Int. 2013 Mar;111(3 Pt B):E54-8. doi: 10.1111/j.1464-410X.2012.11435.x. Epub 2012 Oct 8. BJU Int. 2013. PMID: 23039377
-
Oncology: the role of partial nephrectomy in Wilms tumor.Curr Urol Rep. 2013 Aug;14(4):350-8. doi: 10.1007/s11934-013-0330-0. Curr Urol Rep. 2013. PMID: 23712752 Review.
Cited by
-
[Surgical concepts in the treatment of Wilms tumor: An update].Urologe A. 2015 Dec;54(12):1784-91. doi: 10.1007/s00120-015-4014-x. Urologe A. 2015. PMID: 26704280 Review. German.
-
Innovations in the management of Wilms' tumor.Ther Adv Urol. 2014 Aug;6(4):165-76. doi: 10.1177/1756287214528023. Ther Adv Urol. 2014. PMID: 25083165 Free PMC article. Review.
-
Multidisciplinary Treatment Strategies for Wilms Tumor: Recent Advances, Technical Innovations and Future Directions.Front Pediatr. 2022 Jul 14;10:852185. doi: 10.3389/fped.2022.852185. eCollection 2022. Front Pediatr. 2022. PMID: 35911825 Free PMC article. Review.
-
Nephron-sparing surgery for Wilms tumor.Front Pediatr. 2023 Jan 20;11:1122390. doi: 10.3389/fped.2023.1122390. eCollection 2023. Front Pediatr. 2023. PMID: 36743884 Free PMC article. Review.
-
Wilms tumor: a review of current surgical controversies.Transl Androl Urol. 2020 Oct;9(5):2382-2392. doi: 10.21037/tau.2020.03.03. Transl Androl Urol. 2020. PMID: 33209711 Free PMC article. Review.
References
-
- Breslow N, Olshan A, Beckwith JB, et al. Epidemiology of Wilms tumor. Med Pediatr Oncol. 1993;21:172–181. - PubMed
-
- Breslow N, Sharples K, Beckwith JB, et al. Prognostic factors in nonmetastatic, favorable histology Wilms’ tumor. Results of the Third National Wilms’ Tumor Study Cancer. 1991;68:2345–2353. - PubMed
-
- Robson C, Churchill BM, Anderson W. The results of radical nephrectomy for renal cell carcinoma. J Urol. 1969;101:297–301. - PubMed
-
- Varan A, Büyükpamukçu N, Çaglar M, et al. Prognostic Significance of Metastatic Site at Diagnosis in Wilms’ Tumor: Results From a Single Center. J Ped Hem Onc. 2005;27:188–191. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
