

Cartilage and meniscal T2 relaxation time as non-invasive biomarker for knee osteoarthritis and cartilage repair procedures
- PMID: 23896316
- PMCID: PMC3929642
- DOI: 10.1016/j.joca.2013.07.012
Cartilage and meniscal T2 relaxation time as non-invasive biomarker for knee osteoarthritis and cartilage repair procedures
Abstract
Objective: The purpose of this work was to review the current literature on cartilage and meniscal T2 relaxation time.
Methods: Electronic searches in PubMed were performed to identify relevant studies about T2 relaxation time measurements as non-invasive biomarker for knee osteoarthritis (OA) and cartilage repair procedures.
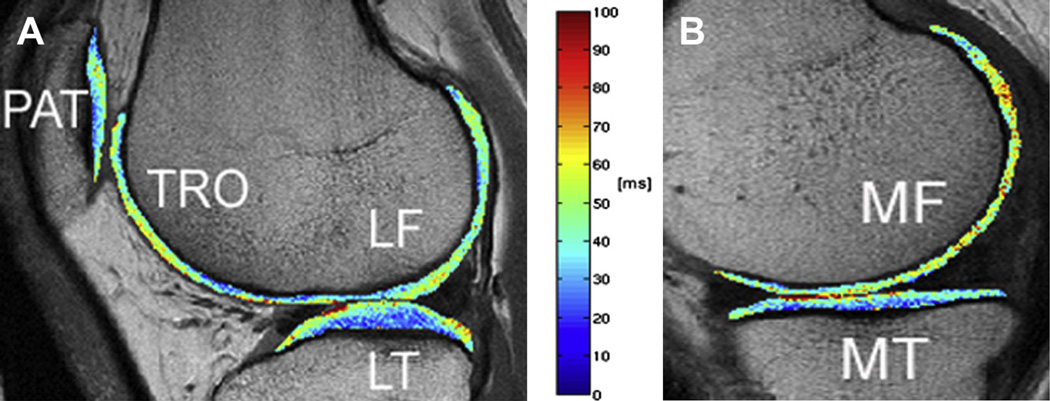
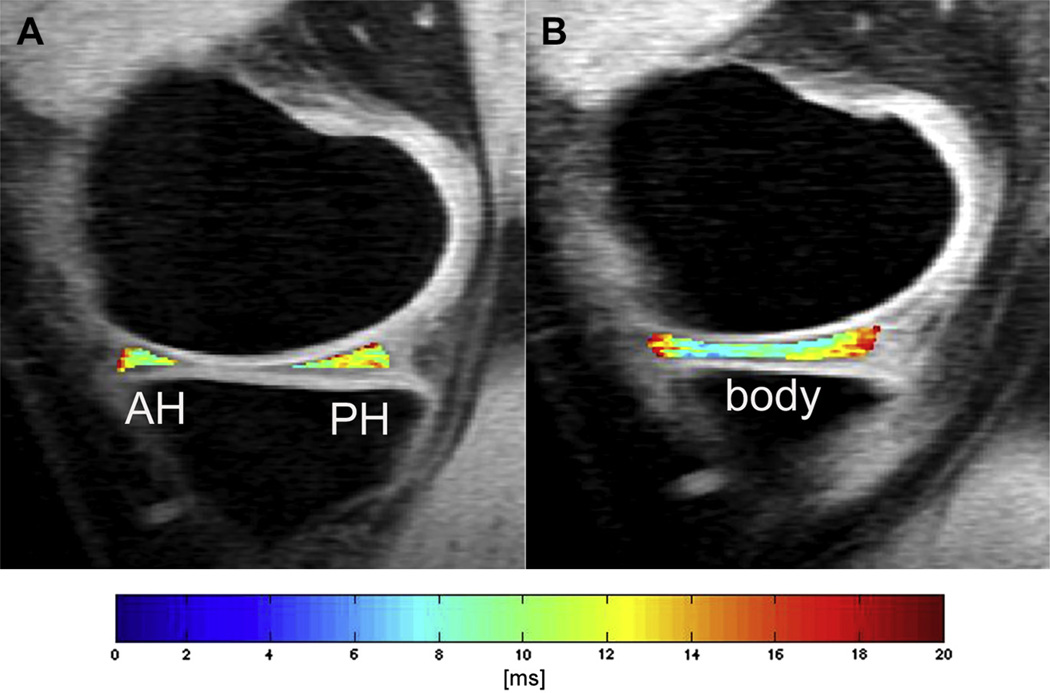
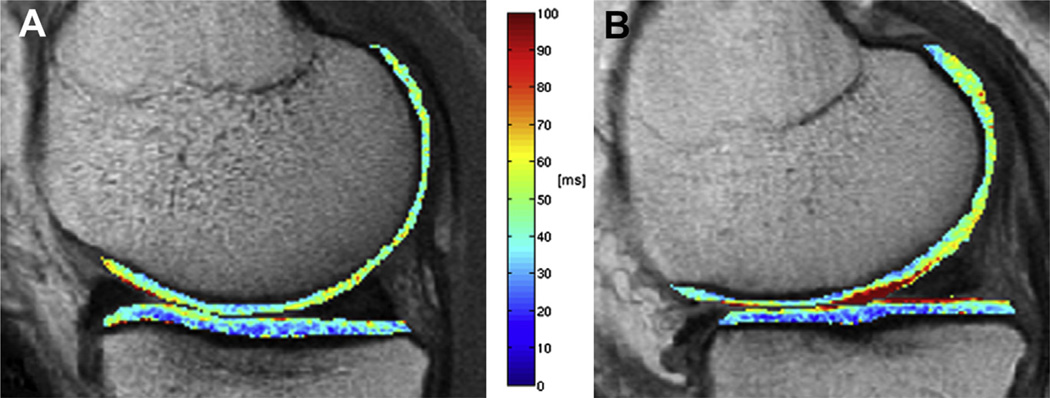
Results: Initial osteoarthritic changes include proteoglycan loss, deterioration of the collagen network, and increased water content within the articular cartilage and menisci. T2 relaxation time measurements are affected by these pathophysiological processes. It was demonstrated that cartilage and meniscal T2 relaxation time values were significantly increased in subjects with compared to those without radiographic OA and focal knee lesions, respectively. Subjects with OA risk factors such as overweight/obesity showed significantly greater cartilage T2 values than normal controls. Elevated cartilage and meniscal T2 relaxation times were found in subjects with vs without knee pain. Increased cartilage T2 at baseline predicted morphologic degeneration in the cartilage, meniscus, and bone marrow over 3 years. Furthermore, cartilage repair tissue could be non-invasively assessed by using T2 mapping. Reproducibility errors for T2 measurements were reported to be smaller than the T2 differences in healthy and diseased cartilage indicating that T2 relaxation time may be a reliable discriminatory biomarker.
Conclusions: Cartilage and meniscal T2 mapping may be suitable as non-invasive biomarker to diagnose early stages of knee OA and to monitor therapy of OA.
Keywords: Cartilage and meniscal T2 relaxation time; Knee; Magnetic resonance imaging; Osteoarthritis.
Copyright © 2013 Osteoarthritis Research Society International. Published by Elsevier Ltd. All rights reserved.
Figures
References
-
- Dijkgraaf LC, de Bont LG, Boering G, Liem RS. Normal cartilage structure, biochemistry, and metabolism: a review of the literature. J Oral Maxillofac Surg. 1995;53:924–929. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
