

Reduction in Framingham risk of cardiovascular disease in obese patients undergoing laparoscopic adjustable gastric banding
- PMID: 23897217
- PMCID: PMC3747322
- DOI: 10.1007/s12325-013-0045-0
Reduction in Framingham risk of cardiovascular disease in obese patients undergoing laparoscopic adjustable gastric banding
Abstract
Background: Obesity is a major risk factor for cardiovascular disease (CVD), with weight loss offering improvement in CVD risk factors.
Aims: To examine whether weight loss in laparoscopic adjustable gastric band (LAGB)-treated obese patients is associated with meaningful reductions in estimated 10- and 30- year Framingham CVD risk 12-15 months post-LAGB.
Methods: Obese adult patients [body mass index (BMI) ≥30 kg/m²] treated with LAGB were identified in a large US healthcare database. Patients without CVD at baseline and with measures of BMI, systolic blood pressure, diabetes, and smoking status at baseline and follow-up were eligible. Non-LAGB patients were propensity score matched to LAGB patients on baseline BMI, age, and gender. Estimated 10- and 30-year risk of developing CVD using office-based data, including BMI, was calculated at baseline and 12-15 months follow-up.
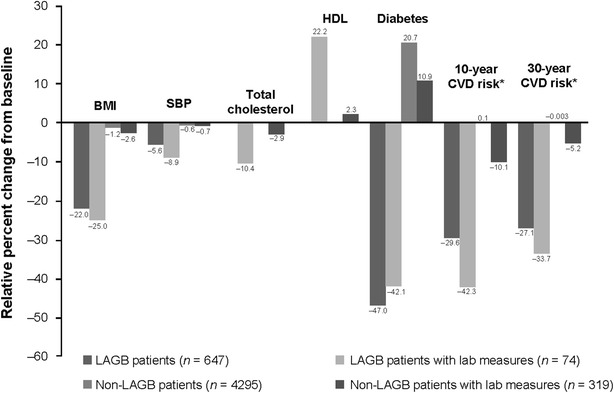
Results: Mean BMI in LAGB patients (n = 647, average age 45.66 years, 81.1% female) decreased from 42.7 to 33.4 kg/m² (P < 0.0001), with 35.4% no longer obese; 10- and 30-year estimated CVD risk decreased from 10.8 to 7.6% (P < 0.0001) and 44.34 to 32.30% (P < 0.0001), respectively, 12-15 months post-LAGB. Improvements were significantly greater than in non-LAGB patients (N = 4,295) (P < 0.0001). In the subset with lipid data (n = 74), improvements in total (-20.6 mg/dL; P < 0.05) and high-density lipoprotein (+10.6 mg/dL, P < 0.0001) cholesterol 1 year post-LAGB were also observed.
Conclusions: Data from a US healthcare database show that individuals undergoing LAGB have significant weight loss and reductions in estimated 10- to 30-year CVD risk within 1 year post-LAGB.
Figures


References
-
- Roger VL, Go AS, Lloyd-Jones DM, American Heart Association Statistical Committee and Stroke Statistics Committee et al. Heart disease and stroke statistics—2011 update: a report from the American Heart Association. Circulation. 2011;123:e18–e209. doi: 10.1161/CIR.0b013e3182009701. - DOI - PMC - PubMed
-
- Heidenreich PA, Trogdon JG, Khavjou OA, The American Heart Association Advocacy Coordinating Committee. Stroke Council. Council on Cardiovascular Radiology and Intervention. Council on Clinical Cardiology. Council on Epidemiology and Prevention. Council on Arteriosclerosis, Thrombosis and Vascular Biology. Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation. Council on Cardiovascular Nursing. Council on the Kidney in Cardiovascular Disease. Council on Cardiovascular Surgery and Anesthesia. Interdisciplinary Council on Quality of Care and Outcomes Research et al. Forecasting the future of cardiovascular disease in the United States: a policy statement from the American Heart Association. Circulation. 2011;123:933–944. doi: 10.1161/CIR.0b013e31820a55f5. - DOI - PubMed
-
- CDC/NCHS. National Health and Nutrition Examination Survey Data. Centers for Disease Control and Prevention (CDC) and National Center for Health Statistics (NCHS) 2011. Available at http://www.cdc.gov/nchs/nhanes/nhanes_questionnaires.htm. Last accessed 25 April 2012.
-
- Poirier P, Giles TD, Bray GA, American Heart Association Obesity Committee of the Council on Nutrition, Physical Activity, and Metabolism et al. Obesity and cardiovascular disease: pathophysiology, evaluation, and effect of weight loss: an update of the 1997 American Heart Association Scientific Statement on Obesity and Heart Disease from the Obesity Committee of the Council on Nutrition, Physical Activity, and Metabolism. Circulation. 2006;2006(113):898–918. doi: 10.1161/CIRCULATIONAHA.106.171016. - DOI - PubMed
-
- Dattilo AM, Kris-Etherton PM. Effects of weight reduction on blood lipids and lipoproteins: a meta-analysis. Am J Clin Nutr. 1992;56:320–328. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
