

Upper gastrointestinal bleeding in cirrhosis: varix or no varix?
- PMID: 23897373
- PMCID: PMC3736272
- DOI: 10.1136/bcr-2013-008815
Upper gastrointestinal bleeding in cirrhosis: varix or no varix?
Abstract
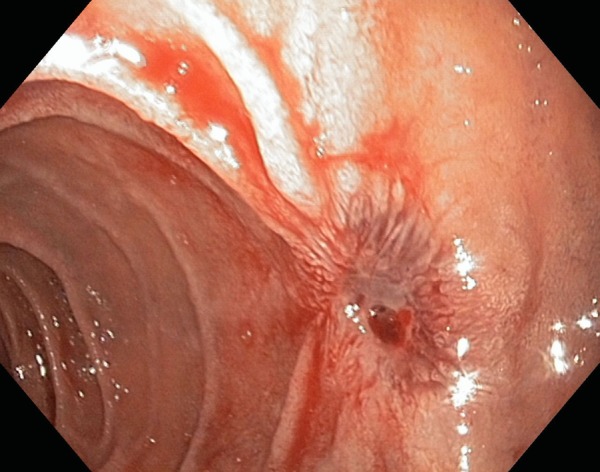
Upper gastrointestinal bleeding from variceal origin is a frequent complication in the cirrhotic population. Duodenal variceal haemorrhage, however, is infrequent and the endoscopic management of such lesions is not straightforward. Non-endoscopic options include vasoactive drugs, transjugular intrahepatic portosystemic shunt (TIPS), transvenous obliteration and surgery as rescue therapy. We present a patient with Child-Pugh A hepatitis C virus-cirrhosis with acute bleeding from a duodenal varix. It was managed with elastic band ligation but late rebleeding occurred after 6 weeks. Gastroduodenoscopy revealed active bleeding from the ligation eschar. Band ligation and sclerosis were attempted but unsuccessful. Terlipressin was started and the patient referred for TIPS. Surprisingly, angiography showed a normal hepatic vein pressure gradient; therefore, TIPS was not performed. Haemorrhage ceased with medical treatment alone. The patient remained stable and was discharged after 10 days, being currently under evaluation for hepatitis C therapy.
Figures




Similar articles
-
Medical management of variceal bleeding in patients with cirrhosis.Can J Gastroenterol. 2004 Feb;18(2):109-13. doi: 10.1155/2004/560215. Can J Gastroenterol. 2004. PMID: 14997222 Review.
-
Early TIPS with covered stents versus standard treatment for acute variceal bleeding in patients with advanced cirrhosis: a randomised controlled trial.Lancet Gastroenterol Hepatol. 2019 Aug;4(8):587-598. doi: 10.1016/S2468-1253(19)30090-1. Epub 2019 May 29. Lancet Gastroenterol Hepatol. 2019. PMID: 31153882 Clinical Trial.
-
[A prospective study comparing the efficacy of early administration of terlipressin and somatostatin for the control of acute variceal bleeding in patients with cirrhosis].Korean J Hepatol. 2006 Sep;12(3):373-84. Korean J Hepatol. 2006. PMID: 16998289 Clinical Trial. Korean.
-
Terlipressin vs. octreotide in bleeding esophageal varices as an adjuvant therapy with endoscopic band ligation: a randomized double-blind placebo-controlled trial.Am J Gastroenterol. 2009 Mar;104(3):617-23. doi: 10.1038/ajg.2008.147. Epub 2009 Feb 17. Am J Gastroenterol. 2009. PMID: 19223890 Clinical Trial.
-
Acute variceal bleeding.Semin Respir Crit Care Med. 2012 Feb;33(1):46-54. doi: 10.1055/s-0032-1301734. Epub 2012 Mar 23. Semin Respir Crit Care Med. 2012. PMID: 22447260 Review.
Cited by
-
Haemorrhagic shock leading to death due to ruptured esophageal varices: An autopsy based case report.Ann Med Surg (Lond). 2022 Jun 4;78:103932. doi: 10.1016/j.amsu.2022.103932. eCollection 2022 Jun. Ann Med Surg (Lond). 2022. PMID: 35734713 Free PMC article.
-
The challenge of triple intestinal parasite infections in immigrants-A call for comprehensive differential diagnosis.Clin Case Rep. 2024 Nov 6;12(11):e9549. doi: 10.1002/ccr3.9549. eCollection 2024 Nov. Clin Case Rep. 2024. PMID: 39512789 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical