

JURaSSiC: accuracy of clinician vs risk score prediction of ischemic stroke outcomes
- PMID: 23897872
- PMCID: PMC3776534
- DOI: 10.1212/WNL.0b013e31829d874e
JURaSSiC: accuracy of clinician vs risk score prediction of ischemic stroke outcomes
Abstract
Objective: We compared the accuracy of clinicians and a risk score (iScore) to predict observed outcomes following an acute ischemic stroke.
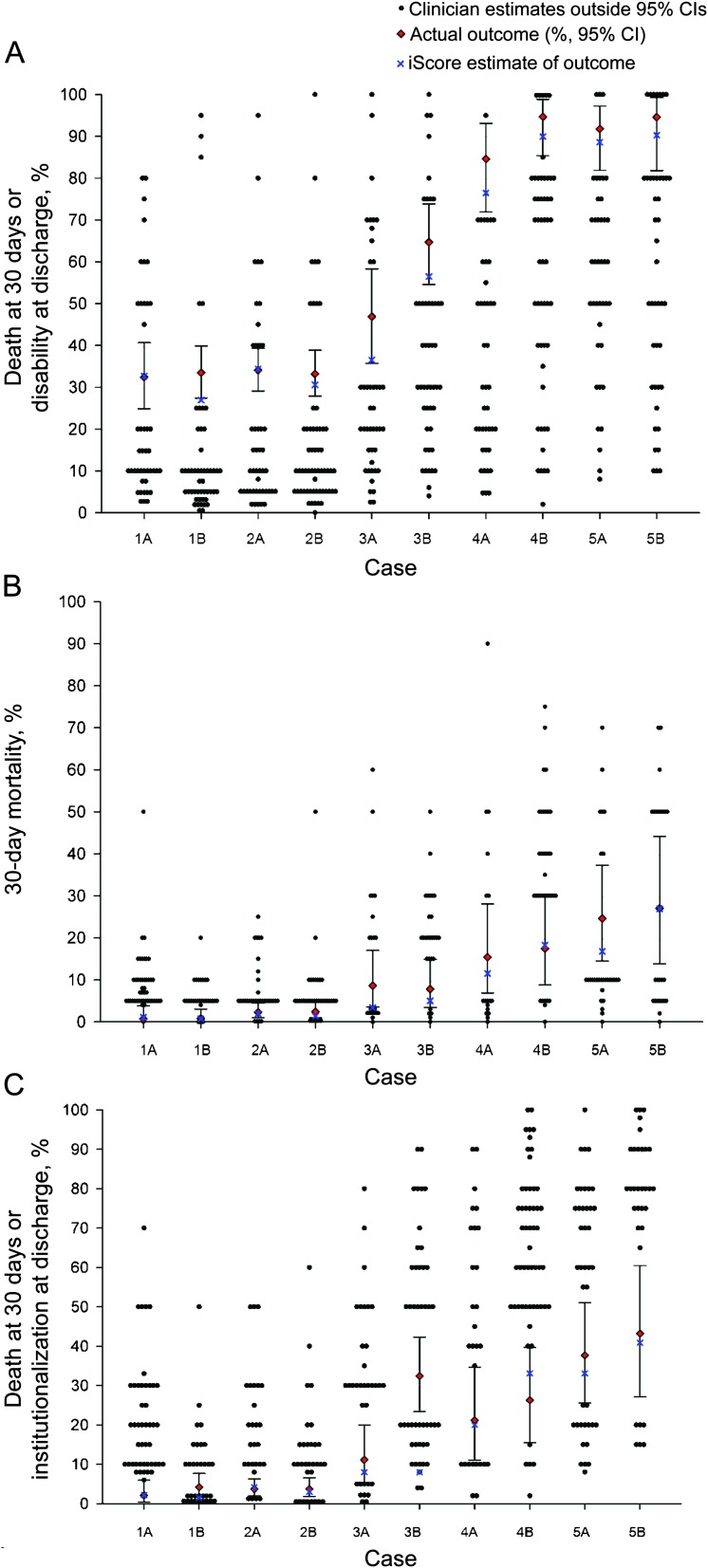
Methods: The JURaSSiC (Clinician JUdgment vs Risk Score to predict Stroke outComes) study assigned 111 clinicians with expertise in acute stroke care to predict the probability of outcomes of 5 ischemic stroke case scenarios. Cases (n = 1,415) were selected as being representative of the 10 most common clinical presentations from a pool of more than 12,000 stroke patients admitted to 12 stroke centers. The primary outcome was prediction of death or disability (modified Rankin Scale [mRS] ≥3) at discharge within the 95% confidence interval (CI) of observed outcomes. Secondary outcomes included 30-day mortality and death or institutionalization at discharge.
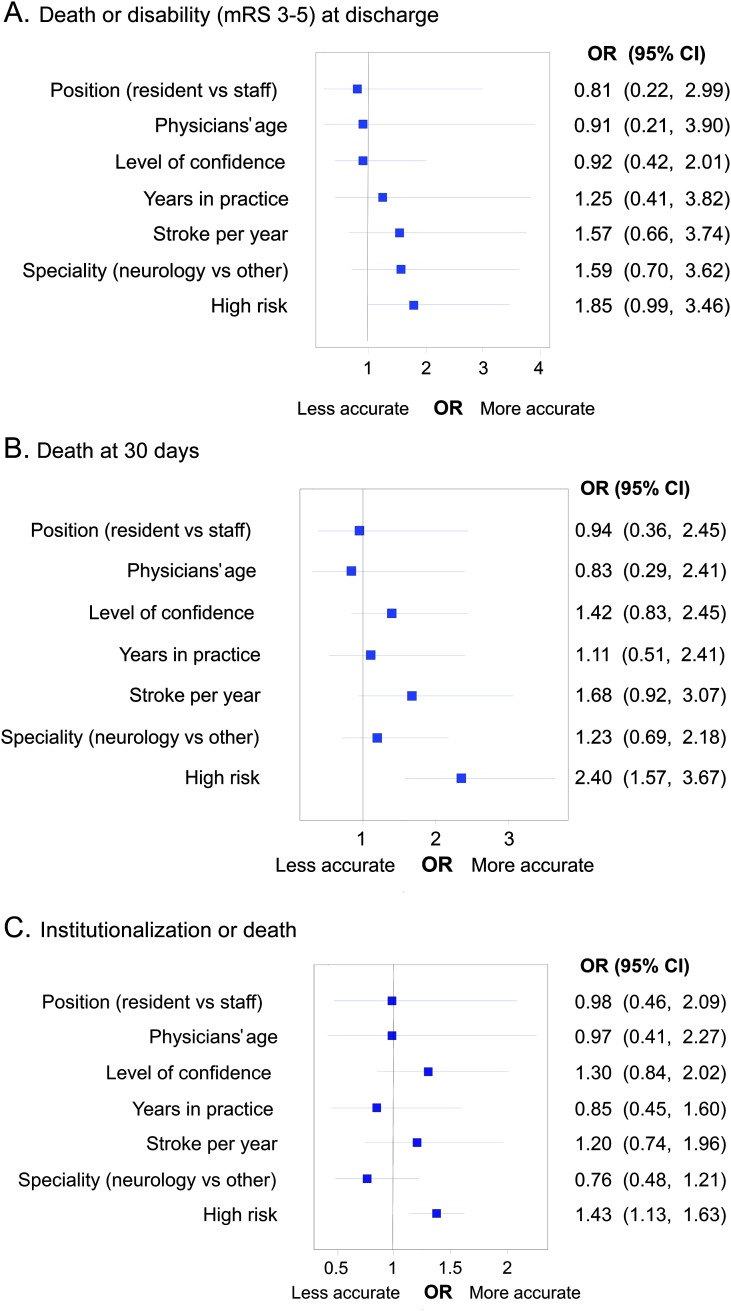
Results: Clinicians made 1,661 predictions with overall accuracy of 16.9% for death or disability at discharge, 46.9% for 30-day mortality, and 33.1% for death or institutionalization at discharge. In contrast, 90% of the iScore-based estimates were within the 95% CI of observed outcomes. Nearly half (n = 53 of 111; 48%) of participants were unable to accurately predict the probability of the primary outcome in any of the 5 rated cases. Less than 1% (n = 1) provided accurate predictions in 4 of the 5 cases and none accurately predicted all 5 case outcomes. In multivariable analyses, the presence of patient characteristics associated with poor outcomes (mRS ≥3 or death) in previous studies (older age, high NIH Stroke Scale score, and nonlacunar subtype) were associated with more accurate clinician predictions of death at 30 days (odds ratio [OR] 2.40, 95% CI 1.57-3.67) and with a trend for more accurate predictions of death or disability at discharge (OR 1.85, 95% CI 0.99-3.46).
Conclusions: Clinicians with expertise in stroke performed poorly compared to a validated tool in predicting the outcomes of patients with an acute ischemic stroke. Use of the risk stroke outcome tool may be superior for decision-making following an acute ischemic stroke.
Figures
References
-
- Nichols-Larsen DS, Clark PC, Zeringue A, Greenspan A, Blanton S. Factors influencing stroke survivors' quality of life during subacute recovery. Stroke 2005;36:1480–1484 - PubMed
-
- Langhorne P, Coupar F, Pollock A. Motor recovery after stroke: a systematic review. Lancet Neurol 2009;8:741–754 - PubMed
-
- Solberg OG, Dahl M, Mowinckel P, Stavem K. Derivation and validation of a simple risk score for predicting 1-year mortality in stroke. J Neurol 2007;254:1376–1383 - PubMed
-
- Friberg J, Scharling H, Gadsboll N, Truelsen T, Jensen GB. Comparison of the impact of atrial fibrillation on the risk of stroke and cardiovascular death in women versus men (The Copenhagen City Heart Study). Am J Cardiol 2004;94:889–894 - PubMed
-
- Saposnik G, Young B, Silver B, et al. Lack of improvement in patients with acute stroke after treatment with thrombolytic therapy: predictors and association with outcome. JAMA 2004;292:1839–1844 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical