

Patterns of Recurrence and outcome according to breast cancer subtypes in lymph node-negative disease: results from international breast cancer study group trials VIII and IX
- PMID: 23897954
- PMCID: PMC3753700
- DOI: 10.1200/JCO.2012.46.1574
Patterns of Recurrence and outcome according to breast cancer subtypes in lymph node-negative disease: results from international breast cancer study group trials VIII and IX
Abstract
Purpose: To retrospectively evaluate the pattern of recurrence and outcome of node-negative breast cancer (BC) according to major subtypes.
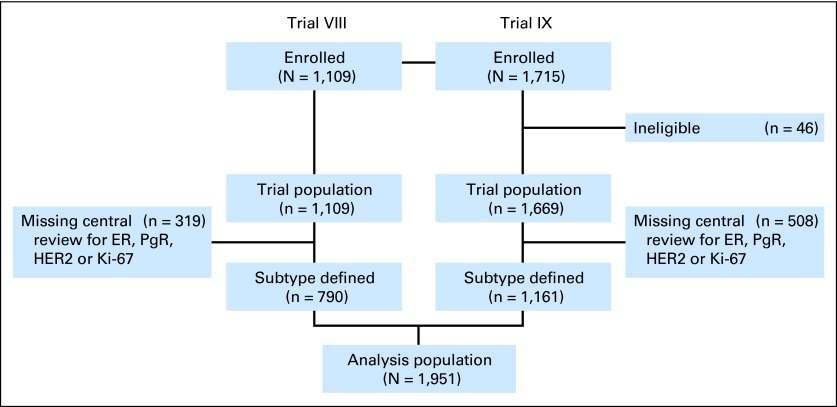
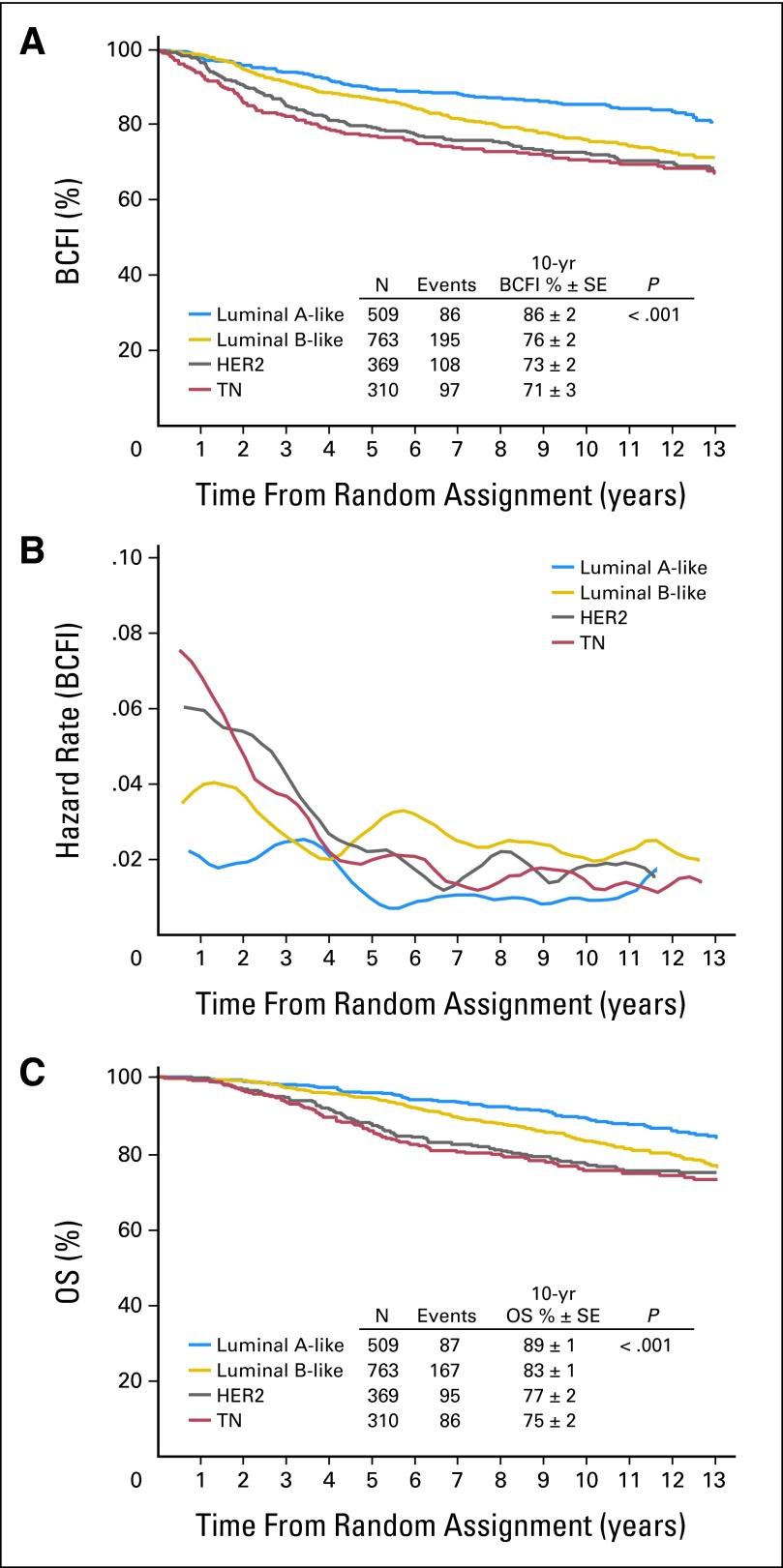
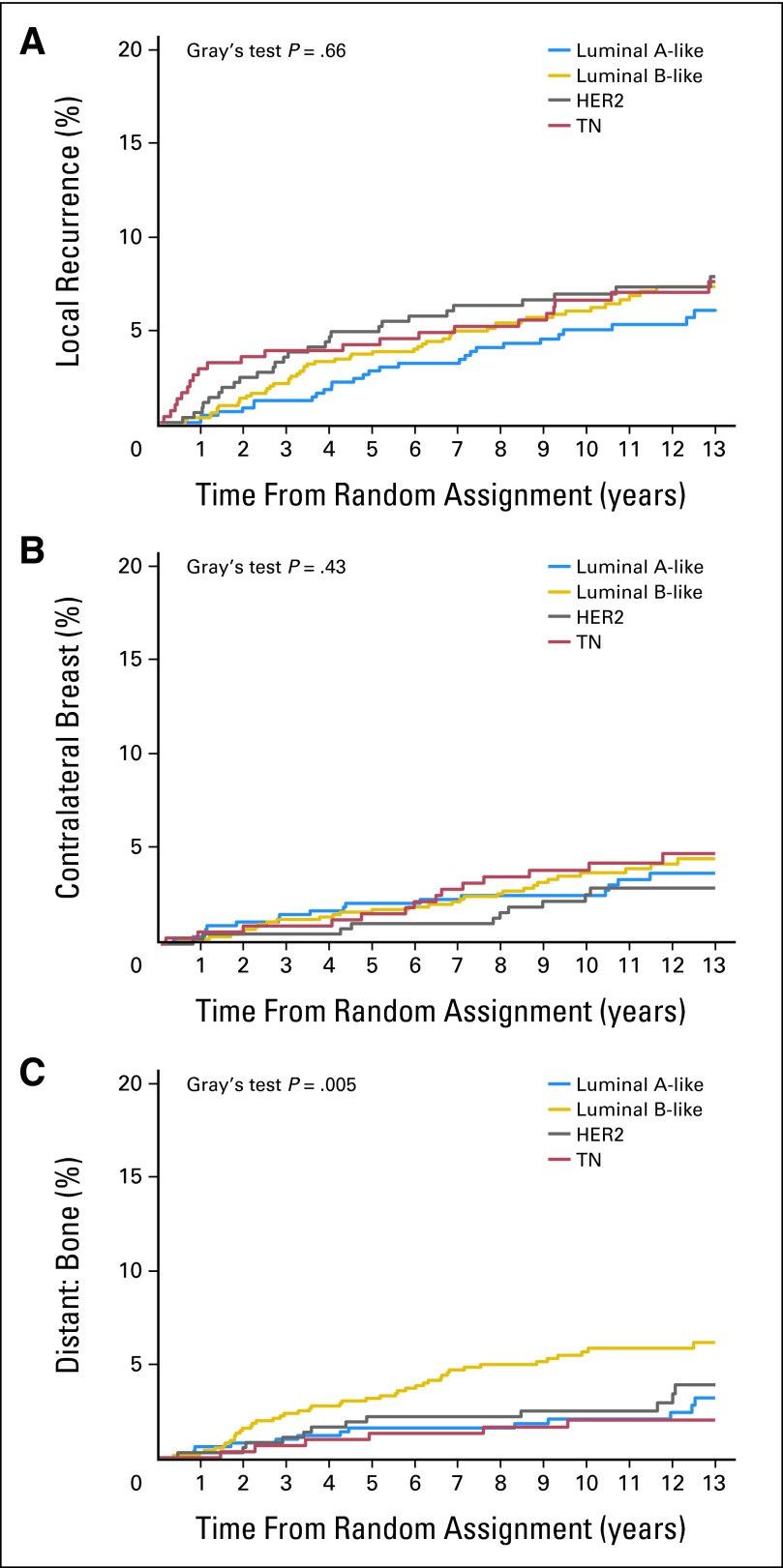
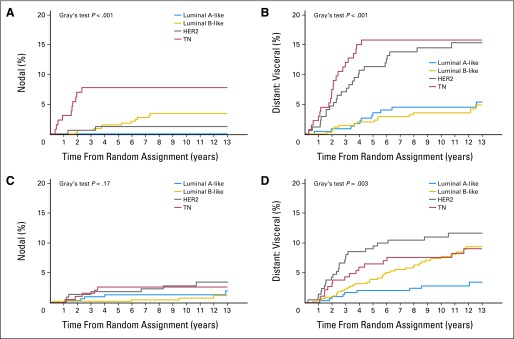
Patients and methods: In all, 1,951 patients with node-negative, early-stage BC randomly assigned in International Breast Cancer Study Group Trials VIII and IX with centrally reviewed pathology data were included. BC subtypes were defined as triple negative (TN; n = 310), human epidermal growth factor receptor 2 (HER2) positive (n = 369), and hormone receptor positive with high (luminal B-like [LB-like]; n = 763) or low (luminal A-like [LA-like]; n = 509) proliferative activity by Ki-67 labeling index. BC-free interval (BCFI) events were invasive BC recurrence in local, contralateral breast, nodal, bone, or visceral sites. Time to first site-specific recurrence was evaluated by using cumulative incidence and competing risks regression analysis.
Results: Median follow-up was 12.5 years. The 10-year BCFI was higher for patients with LA-like (86%) BC compared with LB-like (76%), HER2 (73%), and TN (71%; P < .001) BC. TN and HER2 cohorts had higher hazard of BCFI event in the first 4 years after diagnosis (pre-trastuzumab). LB-like cohorts had a continuously higher hazard of BCFI event over time compared with LA-like cohorts. Ten-year overall survival was higher for LA-like (89%) compared with LB-like (83%), HER2 (77%), and TN (75%; P < .001) BC. LB-like subtypes had higher rates of bone as first recurrence site than other subtypes (P = .005). Visceral recurrence as first site was lower for the LA-like subgroup, with similar incidence among the other subgroups when treated with chemotherapy (P = .003).
Conclusion: BC subtypes have different distant recurrence patterns over time. Defining different patterns of BC recurrence can improve BC care through surveillance guidelines and can guide the design of clinical studies.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
References
-
- Early Breast Cancer Trialists' Collaborative Group (EBCTCG) Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: An overview of the randomised trials. Lancet. 2005;365:1687–1717. - PubMed
-
- Pestalozzi BC, Zahrieh D, Price KN, et al. Identifying breast cancer patients at risk for central nervous system (CNS) metastases in trials of the International Breast Cancer Study Group (IBCSG) Ann Oncol. 2006;17:935–944. - PubMed
-
- Saphner T, Tormey DC, Gray R. Annual hazard rates of recurrence for breast cancer after primary therapy. J Clin Oncol. 1996;14:2738–2746. - PubMed
-
- Grann VR, Troxel AB, Zojwalla NJ, et al. Hormone receptor status and survival in a population-based cohort of patients with breast carcinoma. Cancer. 2005;103:2241–2251. - PubMed
-
- Kennecke H, Yerushalmi R, Woods R, et al. Metastatic behavior of breast cancer subtypes. J Clin Oncol. 2010;28:3271–3277. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
