

Hematopoietic cell transplantation for systemic mature T-cell non-Hodgkin lymphoma
- PMID: 23897963
- PMCID: PMC3753702
- DOI: 10.1200/JCO.2012.46.0188
Hematopoietic cell transplantation for systemic mature T-cell non-Hodgkin lymphoma
Abstract
Purpose: To analyze outcomes of hematopoietic cell transplantation (HCT) in T-cell non-Hodgkin lymphoma.
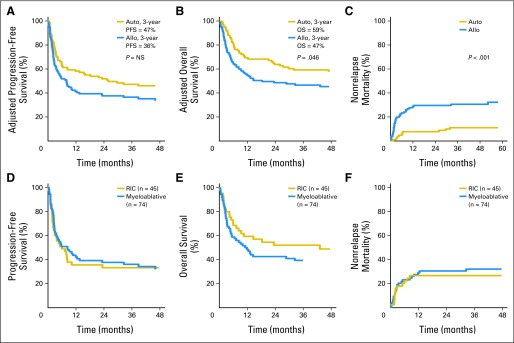
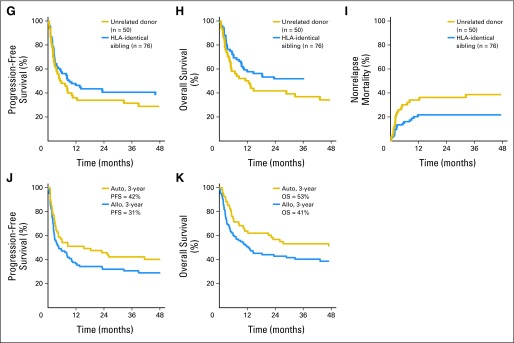
Patients and methods: Outcomes of 241 patients (112 anaplastic large-cell lymphoma, 102 peripheral T-cell lymphoma not otherwise specified, 27 angioimmunoblastic T-cell lymphoma) undergoing autologous HCT (autoHCT; n = 115; median age, 43 years) or allogeneic HCT (alloHCT; n = 126; median age, 38 years) were analyzed. Primary outcomes were nonrelapse mortality (NRM), relapse/progression, progression-free survival (PFS), and overall survival (OS). Patient, disease, and HCT-related variables were analyzed in multivariate Cox proportional hazard models to determine association with outcomes.
Results: AutoHCT recipients were more likely in first complete remission (CR1; 35% v 14%; P = .001) and with chemotherapy-sensitive disease (86% v 60%; P < .001), anaplastic large-cell histology (53% v 40%; P = .04), and two or fewer lines of prior therapy (65% v 44%; P < .001) compared with alloHCT recipients. Three-year PFS and OS of autoHCT recipients beyond CR1 were 42% and 53%, respectively. Among alloHCT recipients who received transplantations beyond CR1, 31% remained progression-free at 3 years, despite being more heavily pretreated and with more refractory disease. NRM was 3.5-fold higher (95% CI, 1.80 to 6.99; P < .001) for alloHCT. In multivariate analysis, chemotherapy sensitivity (hazard ratio [HR], 1.8; 95% CI, 1.16 to 2.87) and two or fewer lines of pretransplantation therapy (HR, 5.02; 95% CI, 2.15 to 11.72) were prognostic of survival.
Conclusion: These data describe the roles of autoHCT and alloHCT in T-cell non-Hodgkin lymphoma and suggest greater effectiveness earlier in the disease course, and limited utility in multiply relapsed disease. Notably, autoHCT at relapse may be a potential option for select patients, particularly those with anaplastic large-cell lymphoma histology.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
References
-
- Vose J, Armitage J, Weisenburger D. International peripheral T-cell and natural killer/T-cell lymphoma study: Pathology findings and clinical outcomes. J Clin Oncol. 2008;26:4124–4130. - PubMed
-
- Schmitz N, Trumper L, Ziepert M, et al. Treatment and prognosis of mature T-cell and NK-cell lymphoma: An analysis of patients with T-cell lymphoma treated in studies of the German High-Grade Non-Hodgkin Lymphoma Study Group. Blood. 2010;116:3418–3425. - PubMed
-
- Kyriakou C, Canals C, Goldstone A, et al. High-dose therapy and autologous stem-cell transplantation in angioimmunoblastic lymphoma: Complete remission at transplantation is the major determinant of Outcome-Lymphoma Working Party of the European Group for Blood and Marrow Transplantation. J Clin Oncol. 2008;26:218–224. - PubMed
-
- Reimer P, Rüdiger T, Geissinger E, et al. Autologous stem-cell transplantation as first-line therapy in peripheral T-cell lymphomas: Results of a prospective multicenter study. J Clin Oncol. 2009;27:106–113. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
