

Diagnostic and prognostic value of presepsin in the management of sepsis in the emergency department: a multicenter prospective study
- PMID: 23899120
- PMCID: PMC4056762
- DOI: 10.1186/cc12847
Diagnostic and prognostic value of presepsin in the management of sepsis in the emergency department: a multicenter prospective study
Abstract
Introduction: Sepsis, severe sepsis and septic shock are common conditions with high mortality. Their early diagnosis in the Emergency Department (ED) is one of the keys to improving survival. Procalcitonin (PCT) has been used as a biomarker in septic patients but has limited specificity and can be elevated in other scenarios of systemic inflammatory response syndrome (SIRS). Soluble CD14 (sCD14) or presepsin is the free fragment of a glycoprotein expressed on monocytes and macrophages. Preliminary reports suggest that levels of presepsin are significantly higher in septic patients than in healthy individuals. The aim of this study is to investigate the diagnostic and prognostic value of presepsin compared to PCT in people presenting at the ED with SIRS and suspected sepsis or septic shock.
Methods: This study was conducted in two major hospitals in Turin, Italy. One hundred six patients presenting to the EDs with suspected sepsis or septic shock were included, and another eighty-three patients affected by SIRS, but with no clinical evidence of infection, were recruited as controls. Blood samples were collected at first medical evaluation and for some patients after 24 and 72 h. The samples were analyzed using the PATHFAST Presepsin assay for sCD14, and commercial kits were used for other determinations (for example, PCT). Definitive diagnosis and survival rates were obtained afterward by analysis of digital medical records.
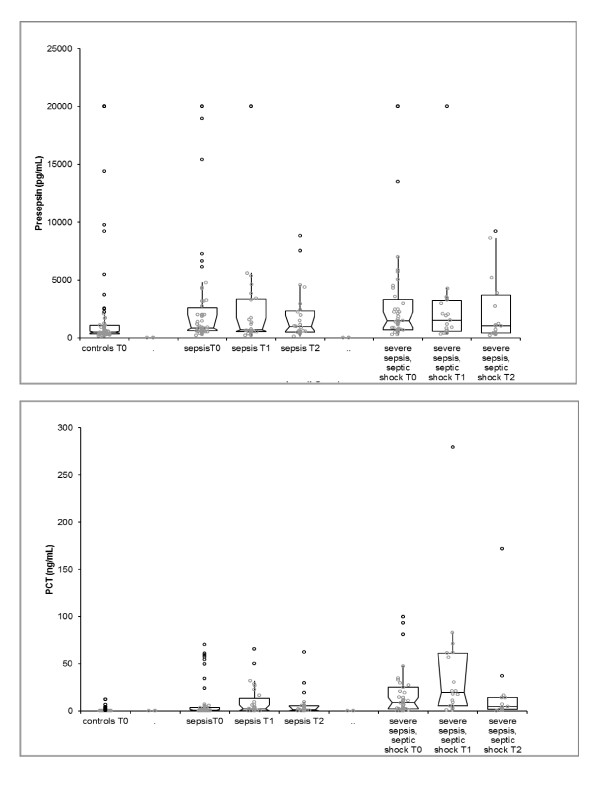
Results: Elevated concentrations of presepsin at presentation were observed in septic patients compared to control patients. The same trend was observed for mean values of PCT. Higher values of presepsin were observed in septic patients at presentation (time 0). The diagnostic accuracy of PCT was generally higher, and areas under the curve (AUCs) were 0.875 for PCT and 0.701 for presepsin. Mean presepsin values were significantly higher in nonsurvivor septic patients (60-day mortality) than in survivors. No significant correlation was noted between PCT and survival.
Conclusions: In our experience, presepsin was useful in the early diagnosis of infection in a complex population of patients with SIRS, sepsis, severe sepsis and septic shock who presented to the ED. Presepsin showed a significant prognostic value, and initial values were significantly correlated with in-hospital mortality of patients affected by sepsis, severe sepsis or septic shock.
Figures


References
-
- Dellinger RP, Levy MM, Rhodes A, Annane D, Gerlach H, Opal SM, Sevransky JE, Sprung CL, Douglas IS, Jaeschke R, Osborn TM, Nunnally ME, Townsend SR, Reinhart K, Kleinpell RM, Angus DC, Deutschman CS, Machado FR, Rubenfeld GD, Webb SA, Beale RJ, Vincent JL, Moreno R. Surviving Sepsis Campaign Guidelines Committee including the Pediatric Subgroup. Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012. Crit Care Med. 2013;17:580–637. doi: 10.1097/CCM.0b013e31827e83af. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
