

Pediatric CT: implementation of ASIR for substantial radiation dose reduction while maintaining pre-ASIR image noise
- PMID: 23901128
- PMCID: PMC4489555
- DOI: 10.1148/radiol.13122578
Pediatric CT: implementation of ASIR for substantial radiation dose reduction while maintaining pre-ASIR image noise
Abstract
Purpose: To determine a comprehensive method for the implementation of adaptive statistical iterative reconstruction (ASIR) for maximal radiation dose reduction in pediatric computed tomography (CT) without changing the magnitude of noise in the reconstructed image or the contrast-to-noise ratio (CNR) in the patient.
Materials and methods: The institutional review board waived the need to obtain informed consent for this HIPAA-compliant quality analysis. Chest and abdominopelvic CT images obtained before ASIR implementation (183 patient examinations; mean patient age, 8.8 years ± 6.2 [standard deviation]; range, 1 month to 27 years) were analyzed for image noise and CNR. These measurements were used in conjunction with noise models derived from anthropomorphic phantoms to establish new beam current-modulated CT parameters to implement 40% ASIR at 120 and 100 kVp without changing noise texture or magnitude. Image noise was assessed in images obtained after ASIR implementation (492 patient examinations; mean patient age, 7.6 years ± 5.4; range, 2 months to 28 years) the same way it was assessed in the pre-ASIR analysis. Dose reduction was determined by comparing size-specific dose estimates in the pre- and post-ASIR patient cohorts. Data were analyzed with paired t tests.
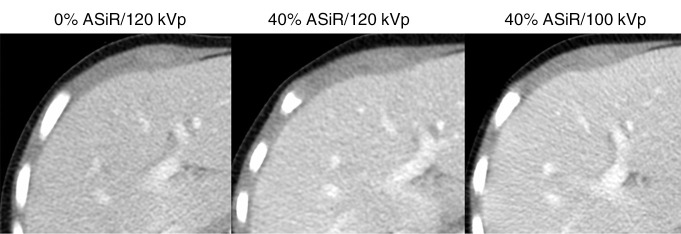
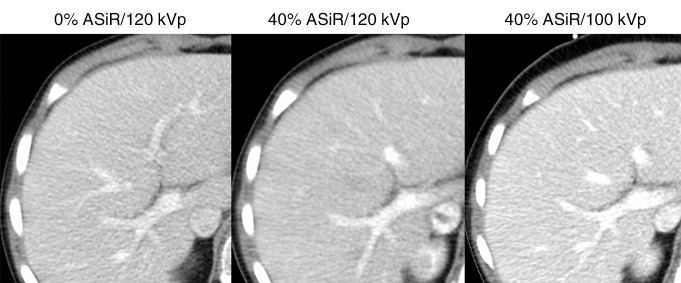
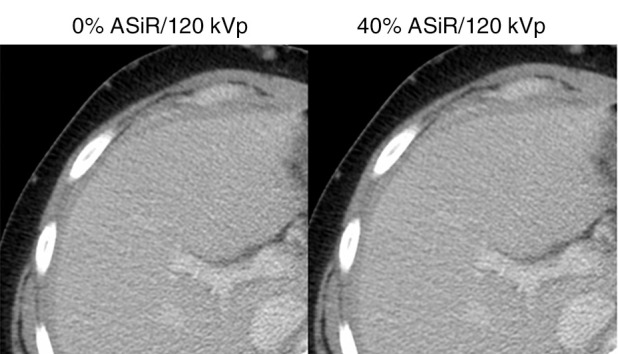
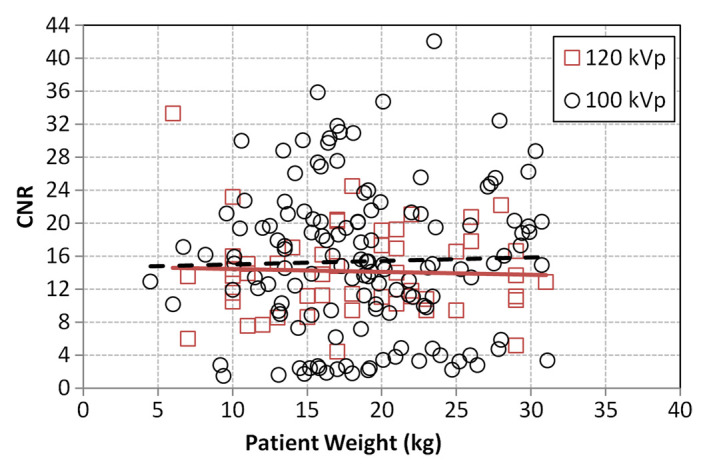
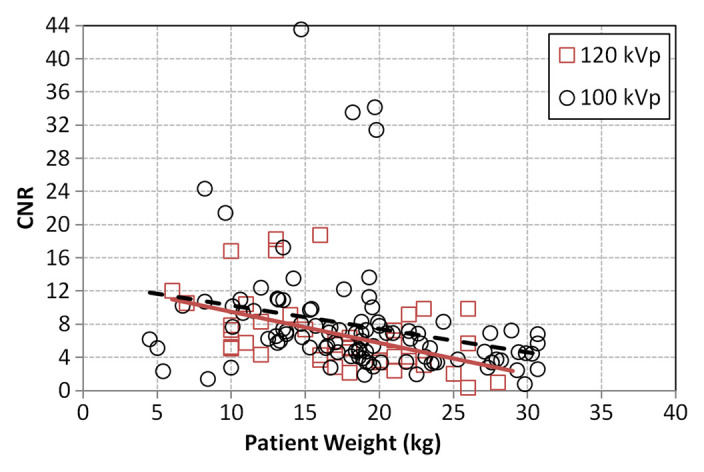
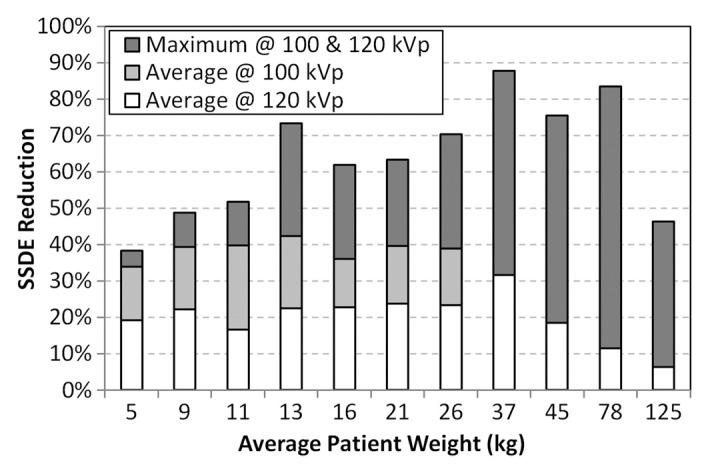
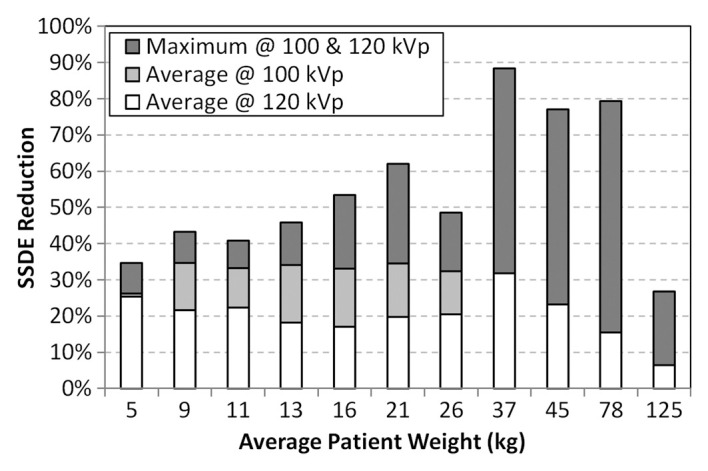
Results: With 40% ASIR implementation, the average relative dose reduction for chest CT was 39% (2.7/4.4 mGy), with a maximum reduction of 72% (5.3/18.8 mGy). The average relative dose reduction for abdominopelvic CT was 29% (4.8/6.8 mGy), with a maximum reduction of 64% (7.6/20.9 mGy). Beam current modulation was unnecessary for patients weighing 40 kg or less. The difference between 0% and 40% ASIR noise magnitude was less than 1 HU, with statistically nonsignificant increases in patient CNR at 100 kVp of 8% (15.3/14.2; P = .41) for chest CT and 13% (7.8/6.8; P = .40) for abdominopelvic CT.
Conclusion: Radiation dose reduction at pediatric CT was achieved when 40% ASIR was implemented as a dose reduction tool only; no net change to the magnitude of noise in the reconstructed image or the patient CNR occurred.
© RSNA, 2013.
Figures
References
-
- Kalra MK , Maher MM , Toth TL , et al. Strategies for CT radiation dose optimization . Radiology 2004. ; 230 ( 3 ): 619 – 628 . - PubMed
-
- Brady SL , Yee BS , Kaufman RA . Characterization of adaptive statistical iterative reconstruction algorithm for dose reduction in CT: a pediatric oncology perspective . Med Phys 2012. ; 39 ( 9 ): 5520 – 5531 . - PubMed
-
- Prakash P , Kalra MK , Digumarthy SR , et al. Radiation dose reduction with chest computed tomography using adaptive statistical iterative reconstruction technique: initial experience . J Comput Assist Tomogr 2010. ; 34 ( 1 ): 40 – 45 . - PubMed
-
- Singh S , Kalra MK , Shenoy-Bhangle AS , et al. Radiation dose reduction with hybrid iterative reconstruction for pediatric CT . Radiology 2012. ; 263 ( 2 ): 537 – 546 . - PubMed
-
- Vorona GA , Ceschin RC , Clayton BL , Sutcavage T , Tadros SS , Panigrahy A . Reducing abdominal CT radiation dose with the adaptive statistical iterative reconstruction technique in children: a feasibility study . Pediatr Radiol 2011. ; 41 ( 9 ): 1174 – 1182 . - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
