

Type-specific diagnosis and evaluation of longitudinal tumor extent of borrmann type IV gastric cancer: CT versus gastroscopy
- PMID: 23901317
- PMCID: PMC3725354
- DOI: 10.3348/kjr.2013.14.4.597
Type-specific diagnosis and evaluation of longitudinal tumor extent of borrmann type IV gastric cancer: CT versus gastroscopy
Abstract
Objective: To compare the accuracy of computed tomography (CT) with that of gastroscopy for the extent of evaluation of longitudinal tumor and type-specific diagnosis of Borrmann type IV gastric cancer.
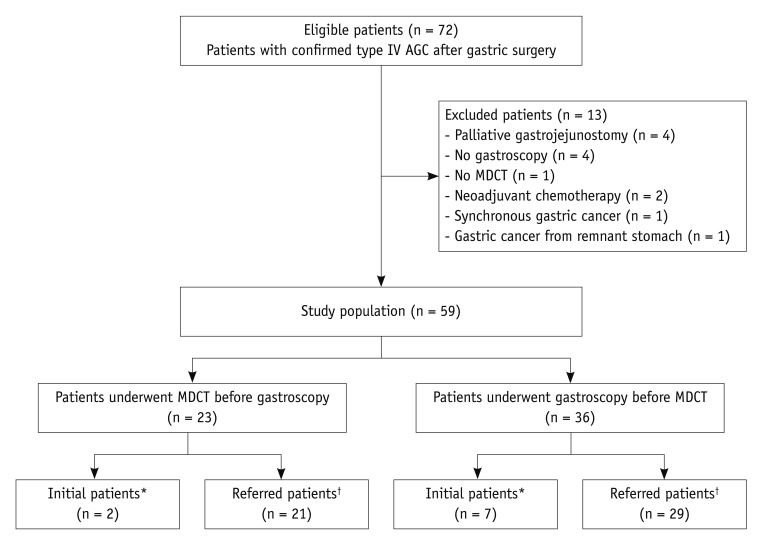
Materials and methods: Fifty-nine patients (35 men with mean age of 60 years and 24 women with mean age of 55 years) who underwent surgical resection of Borrmann type IV gastric cancer were included in this study. Histopathological analysis data was used as a reference standard to confirm the clinical interpretations of gastroscopy and CT for the diagnosis of Borrmann type IV and evaluation of longitudinal tumor extent. For the evaluation of longitudinal extent, gastroscopic and CT results were classified as underestimated, accurate, or overestimated. The McNemar test was used to identify statistically significant differences in the accuracy between gastroscopy and CT.
Results: For the diagnosis of Borrmann type IV gastric cancer, the accuracy of CT was significantly higher than that of gastroscopy (74.6% [44/59] vs. 44.1% [26/59], p < 0.001). CT was significantly more accurate in assessing the overall tumor extent than gastroscopy (61.4% [35/57] vs. 28.1% [16/57], p < 0.001). The proximal (75.4% [43/57] vs. 50.9% [29/57], p = 0.003) and distal tumor extent (71.9% [41/57] vs. 43.9% [25/57], p < 0.05) were more accurately predicted by CT compared with gastroscopy. The underestimation of tumor extent was a major source of error in both examinations.
Conclusion: CT was found to be more predictive than gastroscopy in type-specific diagnosis and the evaluation of longitudinal tumor extent in patients with Borrmann type IV gastric cancer.
Keywords: Borrmann type IV; CT; Cancer; Gastroscopy; Linitis plastica; Stomach.
Figures
References
-
- Nakamura R, Saikawa Y, Wada N, Yoshida M, Kubota T, Kumai K, et al. Retrospective analysis of prognosis for scirrhous-type gastric cancer: one institution's experience. Int J Clin Oncol. 2007;12:291–294. - PubMed
-
- Kim DY, Kim HR, Kim YJ, Kim S. Clinicopathological features of patients with Borrmann type IV gastric carcinoma. ANZ J Surg. 2002;72:739–742. - PubMed
-
- Haruma K, Yoshihara M, Tanaka S, Sumii K, Kajiyama G, Hidaka T, et al. Rapid growth and difficulty of early detection of scirrhous carcinoma of the stomach. Am J Gastroenterol. 1992;87:31–36. - PubMed
-
- Sun XC, Lin J, Ju AH. Treatment of Borrmann type IV gastric cancer with a neoadjuvant chemotherapy combination of docetaxel, cisplatin and 5-fluorouracil/leucovorin. J Int Med Res. 2011;39:2096–2102. - PubMed
-
- Nazli O, Derici H, Tansug T, Yaman I, Bozdag AD, Isgüder AS, et al. Survival analysis after surgical treatment of gastric cancer: review of 121 cases. Hepatogastroenterology. 2007;54:625–629. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
