

Efficacy of remission-induction regimens for ANCA-associated vasculitis
- PMID: 23902481
- PMCID: PMC5953195
- DOI: 10.1056/NEJMoa1213277
Efficacy of remission-induction regimens for ANCA-associated vasculitis
Abstract
Background: The 18-month efficacy of a single course of rituximab as compared with conventional immunosuppression with cyclophosphamide followed by azathioprine in patients with severe (organ-threatening) antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis is unknown.
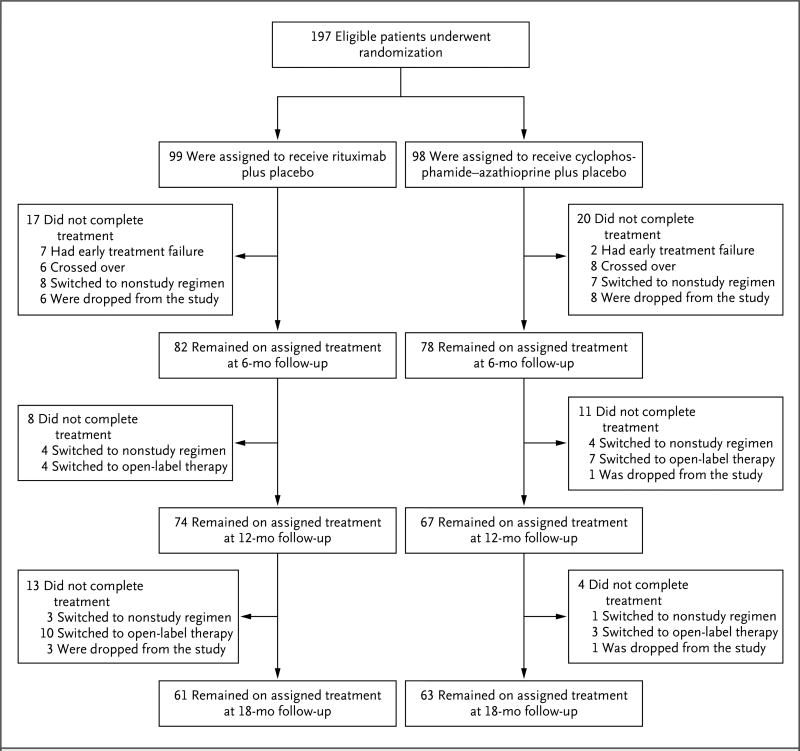
Methods: In a multicenter, randomized, double-blind, double-dummy, noninferiority trial, we compared rituximab (375 mg per square meter of body-surface area administered once a week for 4 weeks) followed by placebo with cyclophosphamide administered for 3 to 6 months followed by azathioprine for 12 to 15 months. The primary outcome measure was complete remission of disease by 6 months, with the remission maintained through 18 months.
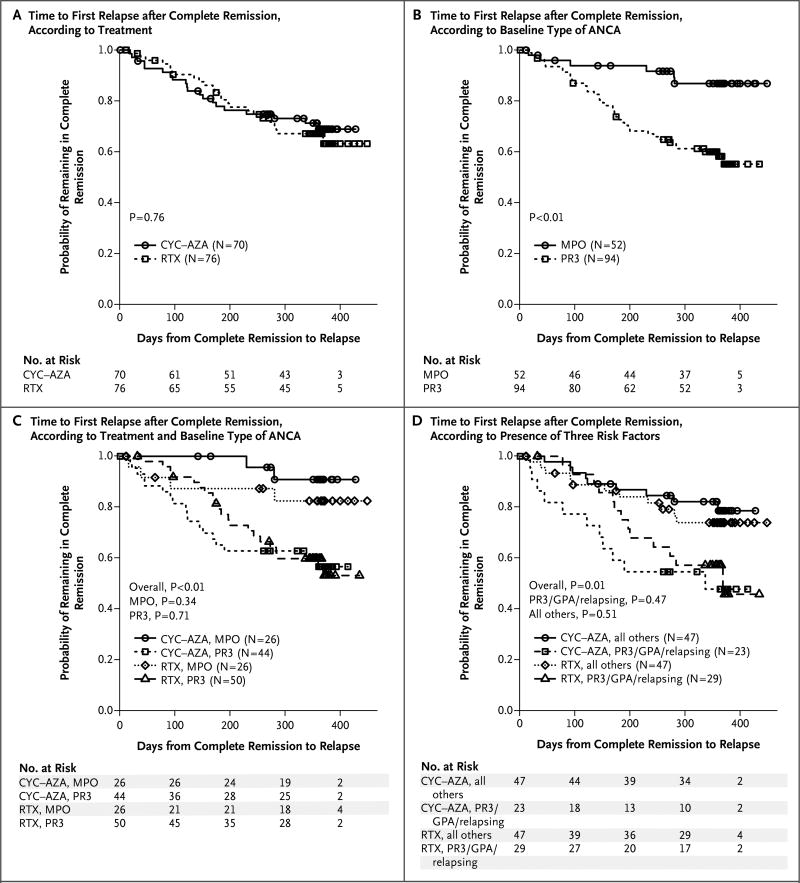
Results: A total of 197 patients were enrolled. As reported previously, 64% of the patients in the rituximab group, as compared with 53% of the patients in the cyclophosphamide-azathioprine group, had a complete remission by 6 months. At 12 and 18 months, 48% and 39%, respectively, of the patients in the rituximab group had maintained the complete remissions, as compared with 39% and 33%, respectively, in the comparison group. Rituximab met the prespecified criteria for noninferiority (P<0.001, with a noninferiority margin of 20%). There was no significant difference between the groups in any efficacy measure, including the duration of complete remission and the frequency or severity of relapses. Among the 101 patients who had relapsing disease at baseline, rituximab was superior to conventional immunosuppression at 6 months (P=0.01) and at 12 months (P=0.009) but not at 18 months (P=0.06), at which time most patients in the rituximab group had reconstituted B cells. There was no significant between-group difference in adverse events.
Conclusions: In patients with severe ANCA-associated vasculitis, a single course of rituximab was as effective as continuous conventional immunosuppressive therapy for the induction and maintenance of remissions over the course of 18 months. (Funded by the National Institute of Allergy and Infectious Diseases and others; RAVE ClinicalTrials.gov number, NCT00104299.)
Figures
Comment in
-
Participant-level data and the new frontier in trial transparency.N Engl J Med. 2013 Aug 1;369(5):468-9. doi: 10.1056/NEJMe1307268. N Engl J Med. 2013. PMID: 23902488 No abstract available.
-
Induction regimens for ANCA-Associated Vasculitis.N Engl J Med. 2013 Nov 7;369(19):1865-6. doi: 10.1056/NEJMc1311108. N Engl J Med. 2013. PMID: 24195565 Free PMC article. No abstract available.
-
Induction regimens for ANCA-Associated Vasculitis.N Engl J Med. 2013 Nov 7;369(19):1864. doi: 10.1056/NEJMc1311108. N Engl J Med. 2013. PMID: 24195566 No abstract available.
-
Induction Regimens for ANCA-Associated Vasculitis.N Engl J Med. 2013 Nov 7;369(19):1864-5. doi: 10.1056/NEJMc1311108. N Engl J Med. 2013. PMID: 24195567 No abstract available.
-
[Effectiveness of regimens of remission-induction on vasculitis associated with antineutrophil cytoplasmic antibodies].Rev Clin Esp (Barc). 2014 Mar;214(2):103. doi: 10.1016/j.rce.2013.09.004. Rev Clin Esp (Barc). 2014. PMID: 24772475 Spanish. No abstract available.
References
-
- Jennette JC, Falk RJ, Andrassy K, et al. Nomenclature of systemic vasculitides: proposal of an international consensus conference. Arthritis Rheum. 1994;37:187–92. - PubMed
-
- Finkielman JD, Lee AS, Hummel AM, et al. ANCA are detectable in nearly all patients with active severe Wegener’s granulomatosis. Am J Med. 2007;120(7):e9–e14. - PubMed
-
- Jones RB, Tervaert JWC, Hauser T, et al. Rituximab versus cyclophosphamide in ANCA-associated renal vasculitis. N Engl J Med. 2010;363:211–20. - PubMed
-
- Hoffman GS, Kerr GS, Leavitt RY, et al. Wegener granulomatosis: an analysis of 158 patients. Ann Intern Med. 1992;116:488–98. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- K24 AR02224/AR/NIAMS NIH HHS/United States
- UL1 RR025005/RR/NCRR NIH HHS/United States
- N01 AI015416/AI/NIAID NIH HHS/United States
- K23 AR052820/AR/NIAMS NIH HHS/United States
- M01 RR000533/RR/NCRR NIH HHS/United States
- UL1 RR025771/RR/NCRR NIH HHS/United States
- K24 AR002224/AR/NIAMS NIH HHS/United States
- UL1 RR024150-01/RR/NCRR NIH HHS/United States
- M01 RR001066/RR/NCRR NIH HHS/United States
- UL1 TR000439/TR/NCATS NIH HHS/United States
- UL1 RR024150/RR/NCRR NIH HHS/United States
- N01-AI-15416/AI/NIAID NIH HHS/United States
- M01 RR00533/RR/NCRR NIH HHS/United States
- K24 AR049185/AR/NIAMS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous