

High rates of death and hospitalization follow bone fracture among hemodialysis patients
- PMID: 23903367
- PMCID: PMC3910091
- DOI: 10.1038/ki.2013.279
High rates of death and hospitalization follow bone fracture among hemodialysis patients
Abstract
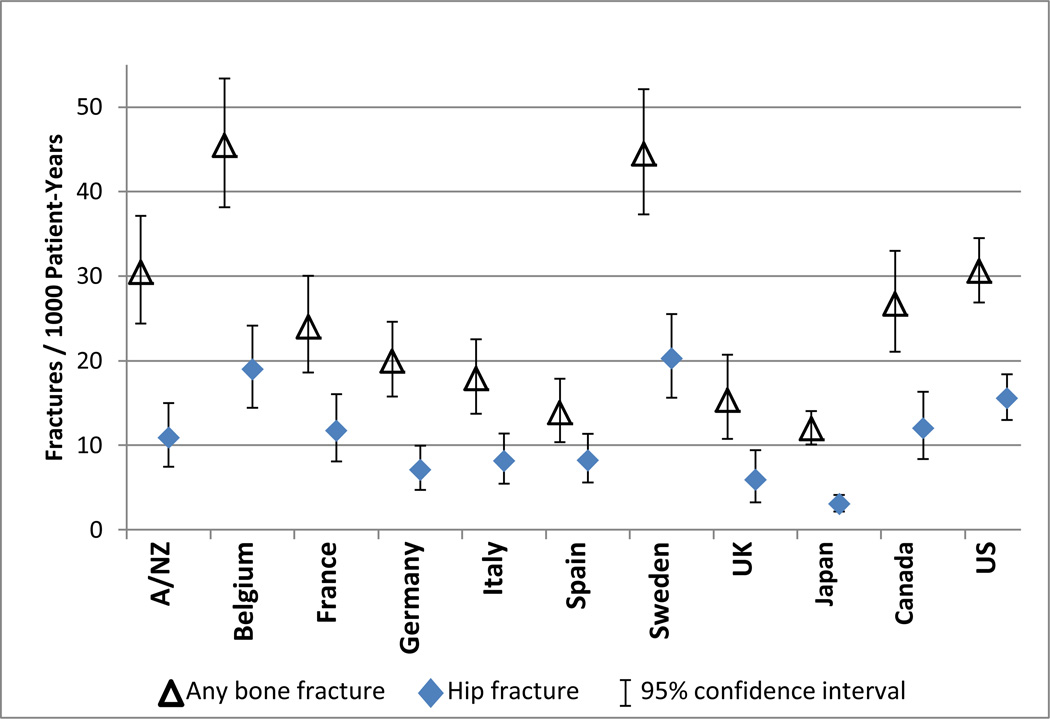
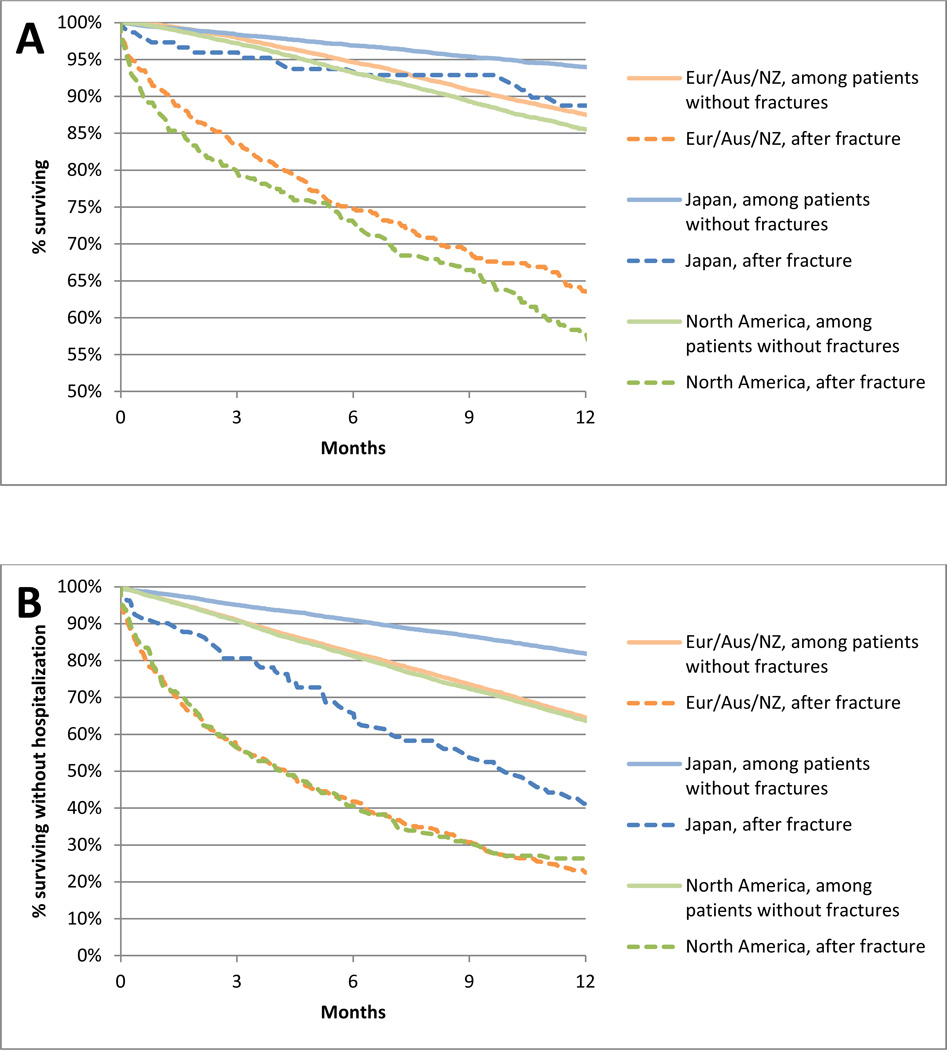
Altered bone structure and function contribute to the high rates of fractures in dialysis patients compared to the general population. Fracture events may increase the risk of subsequent adverse clinical outcomes. Here we assessed the incidence of post-fracture morbidity and mortality in an international cohort of 34,579 in-center hemodialysis patients in the Dialysis Outcomes and Practice Patterns Study (DOPPS). We estimated country-specific rates of fractures requiring a hospital admission and associated length of stay in the hospital. Incidence rates of death and of a composite event of death/rehospitalization were estimated for 1 year after fracture. Overall, 3% of participants experienced a fracture. Fracture incidence varied across countries, from 12 events/1000 patient-years (PY) in Japan to 45/1000 PY in Belgium. In all countries, fracture rates were higher in the hemodialysis group compared to those reported for the general population. Median length of stay ranged from 7 to 37 days in the United States and Japan, respectively. In most countries, postfracture mortality rates exceeded 500/1000 PY and death/rehospitalization rates exceeded 1500/1000 PY. Fracture patients had higher unadjusted rates of death (3.7-fold) and death/rehospitalization (4.0-fold) compared to the overall DOPPS population. Mortality and hospitalization rates were highest in the first month after the fracture and declined thereafter. Thus, the high frequency of fractures and increased adverse outcomes following a fracture pose a significant health burden for dialysis patients. Fracture prevention strategies should be identified and applied broadly in nephrology practices.
Figures




Comment in
-
Fractures in chronic kidney disease: neglected, common, and associated with sickness and death.Kidney Int. 2014 Jan;85(1):20-2. doi: 10.1038/ki.2013.302. Kidney Int. 2014. PMID: 24380905
-
High rates of death and hospitalization follow bone fracture among hemodialysis patients.Kidney Int. 2014 Sep;86(3):649. doi: 10.1038/ki.2014.156. Kidney Int. 2014. PMID: 25168501 No abstract available.
-
The authors reply.Kidney Int. 2014 Sep;86(3):649. doi: 10.1038/ki.2014.160. Kidney Int. 2014. PMID: 25168502 No abstract available.
References
-
- Eckardt KU, Kasiske B. Kidney Disease Improving Global Outcomes (KDIGO): clinical practice guideline for the diagnosis, evaluation, prevention, and treatment of chronic kidney disease-mineral and bone disorder (CKD-MBD) Kidney Int. 2009;76:S1–S130. - PubMed
-
- Coco M, Rush H. Increased incidence of hip fractures in dialysis patients with low serum parathyroid hormone. Am J Kidney Dis. 2000;36:1115–1121. - PubMed
-
- Jadoul M, Albert JM, Akiba T, et al. Incidence and risk factors for hip or other bone fractures among hemodialysis patients in the Dialysis Outcomes and Practice Patterns Study. Kidney Int. 2006;70:1358–1366. - PubMed
-
- Alem AM, Sherrard DJ, Gillen DL, et al. Increased risk of hip fracture among patients with end-stage renal disease. Kidney Int. 2000;58:396–399. - PubMed
-
- Ball AM, Gillen DL, Sherrard D, et al. Risk of hip fracture among dialysis and renal transplant recipients. JAMA. 2002;288:3014–3018. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
