

A cohort study of mortality predictors in patients with acute exacerbation of chronic fibrosing interstitial pneumonia
- PMID: 23903809
- PMCID: PMC3731726
- DOI: 10.1136/bmjopen-2013-002971
A cohort study of mortality predictors in patients with acute exacerbation of chronic fibrosing interstitial pneumonia
Abstract
Objectives: To assess clinical, laboratory and radiographic findings associated with outcomes and to clarify more practical ways to predict hospital mortality in patients with acute exacerbation (AE) of chronic fibrosing interstitial pneumonia (CFIP).
Design: Single-centre retrospective cohort study.
Setting: University Hospital in Japan.
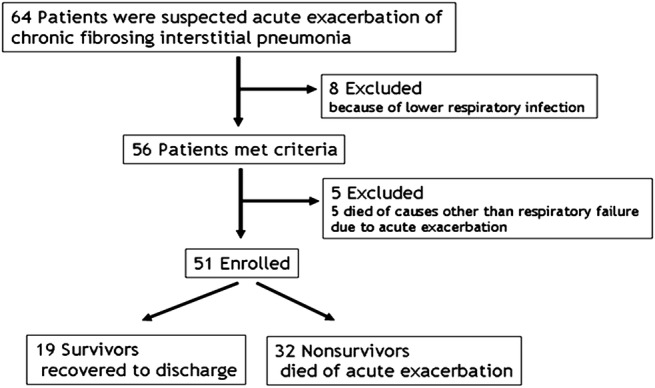
Participants: We identified 51 consecutive patients with AE of idiopathic CFIP through multidisciplinary discussion. Patients who had connective tissue disease, drug-induced lung disease, pneumoconiosis, hypersensitivity pneumonitis, sarcoidosis, pulmonary histiocytosis, lymphangioleiomyomatosis and eosinophilic pneumonia were excluded.
Interventions: There were no interventions.
Main outcome measures: The main outcome was determination of in-hospital mortality predictors. Other outcomes included clinical, laboratory and radiographic differences between non-survivors and survivors in patients with AE of CFIP.
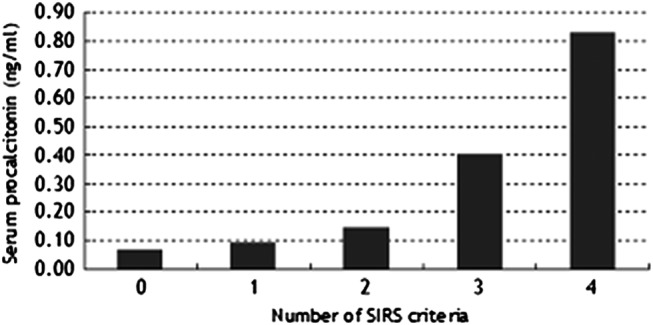
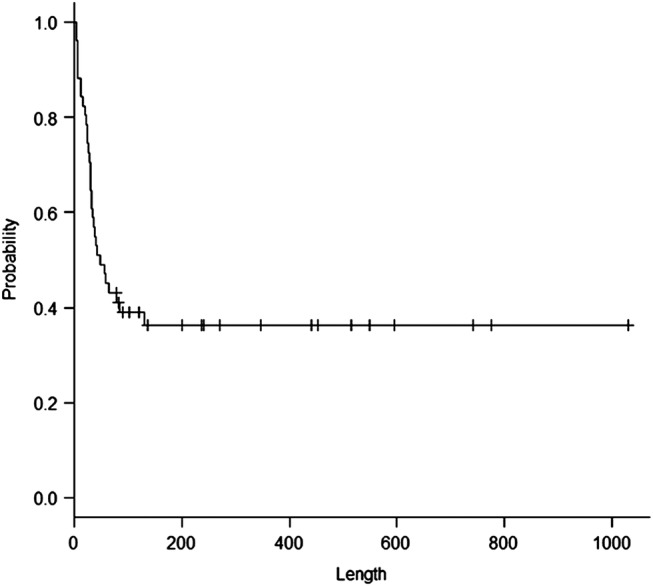
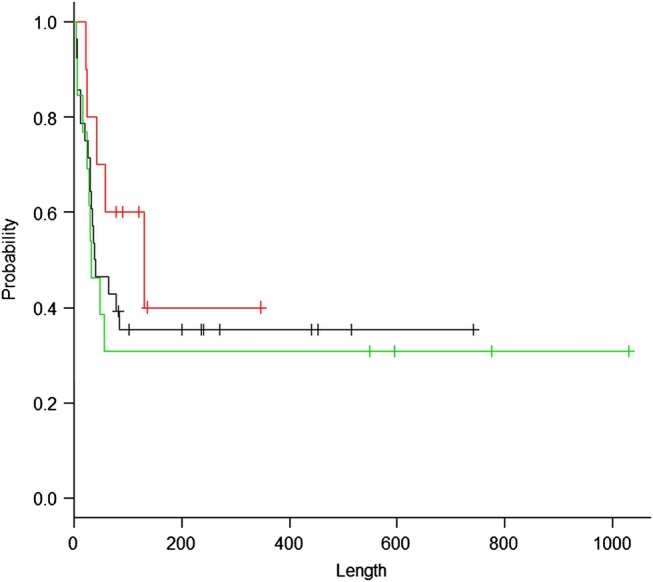
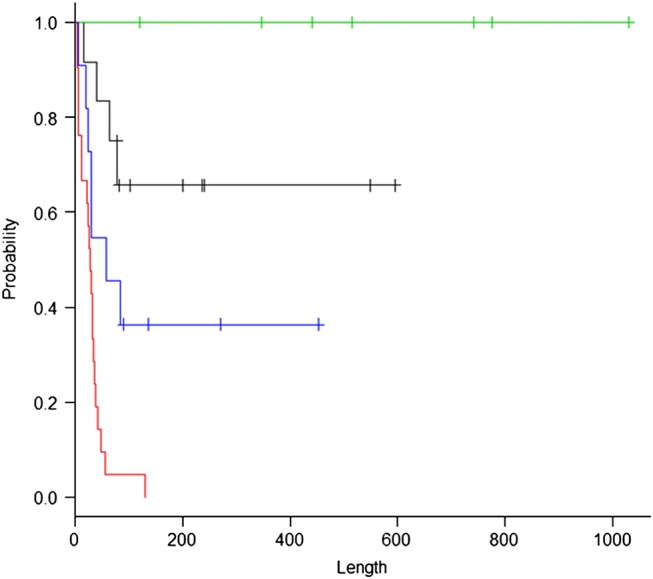
Results: The mean age of the patients with AE of CFIP was 71 years. Compared with survivors, non-survivors had a significantly shorter duration of symptoms before admission, lower prevalence of peripheral distribution of ground-glass opacity and centrilobular emphysema (CLE) on thin-section CT, lower peripheral lymphocyte count, higher brain natriuretic peptide titre, lower Pao2:Fio2 (P:F) ratio, higher prevalence of systemic inflammatory response syndrome (SIRS) and higher SIRS score on admission (p=0.0069, 0.0032, 0.015, 0.040, 0.0098, 0.012, 9.9×10(-7) and 5.4×10(-6), respectively). Multivariate analysis revealed SIRS (HR=6.2810, p=0.015), CLE (HR=0.0606, p=3.6×10(-5)) and serum procalcitonin level (HR=2.7110, p=0.022) to be independent predictors of in-hospital mortality. A Kaplan-Meier estimate on the basis of stratification according to the presence or absence of SIRS and CLE demonstrated a distinct survival curve for each subset of patients.
Conclusions: Distinct survival curves documented by stratification according to the presence or absence of SIRS and CLE may provide basic information for a rational management strategy for patients with AE of CFIP on admission.
Keywords: Centrilobular emphysema; Idiopathic pulmonary fibrosis; Systemic inflammatory response syndrome.
Figures
References
-
- Kondoh Y, Taniguchi H, Kawabata Y, et al. Acute exacerbation in idiopathic pulmonary fibrosis. Analysis of clinical and pathologic findings in three cases. Chest 1993;103:1808–12 - PubMed
-
- Park IN, Kim DS, Shim TS, et al. Acute exacerbation of interstitial pneumonia other than idiopathic pulmonary fibrosis. Chest 2007;132:214–20 - PubMed
-
- Silva CI, Müller NL, Fujimoto K, et al. Acute exacerbation of chronic interstitial pneumonia: high-resolution computed tomography and pathologic findings. J Thorac Imaging 2007;22:221–9 - PubMed
-
- Olson AL, Huie TJ, Groshong SD, et al. Acute exacerbations of fibrotic hypersensitivity pneumonitis: a case series. Chest 2008;134:844–50 - PubMed
-
- Richard L, Kradin RL, Subba R, et al. Case records of the Massachusetts General Hospital. Case 12–2010: an 89-year-old man with progressive dyspnoea. N Engl J Med 2010;362:1522–31 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources