

Meta-analysis of secure randomised controlled trials of β-blockade to prevent perioperative death in non-cardiac surgery
- PMID: 23904357
- PMCID: PMC3932762
- DOI: 10.1136/heartjnl-2013-304262
Meta-analysis of secure randomised controlled trials of β-blockade to prevent perioperative death in non-cardiac surgery
Abstract
Background: Current European and American guidelines recommend the perioperative initiation of a course of β-blockers in those at risk of cardiac events undergoing high- or intermediate-risk surgery or vascular surgery. The Dutch Echocardiographic Cardiac Risk Evaluation Applying Stress Echocardiography (DECREASE) family of trials, the bedrock of evidence for this, are no longer secure. We therefore conducted a meta-analysis of randomised controlled trials of β-blockade on perioperative mortality, non-fatal myocardial infarction, stroke and hypotension in non-cardiac surgery using the secure data.
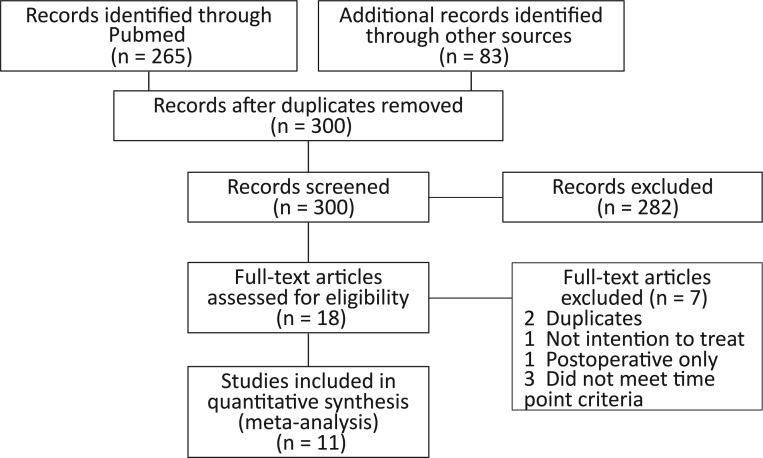
Methods: The randomised controlled trials of initiation of β-blockers before non-cardiac surgery were examined. Primary outcome was all-cause mortality at 30 days or at discharge. The DECREASE trials were separately analysed.
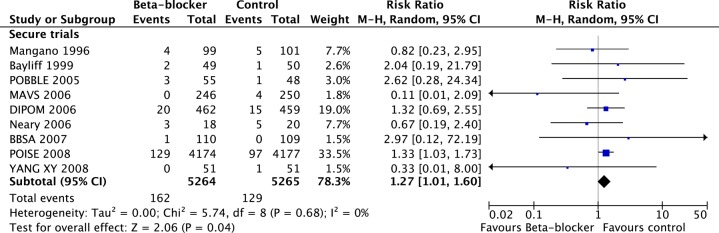
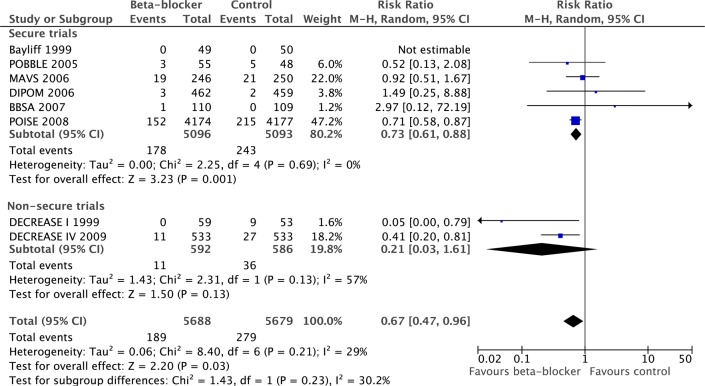
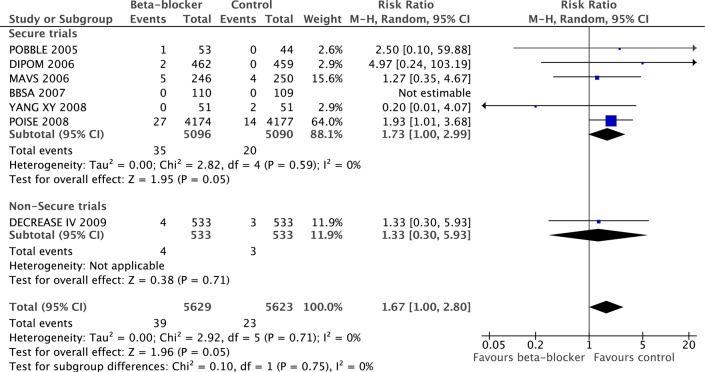
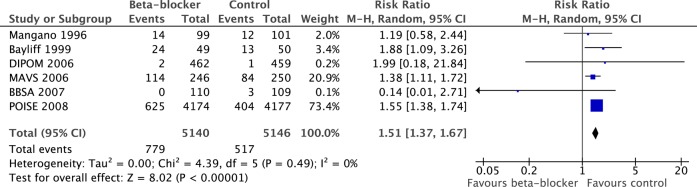
Results: Nine secure trials totalling 10 529 patients, 291 of whom died, met the criteria. Initiation of a course of β-blockers before surgery caused a 27% risk increase in 30-day all-cause mortality (p=0.04). The DECREASE family of studies substantially contradict the meta-analysis of the secure trials on the effect of mortality (p=0.05 for divergence). In the secure trials, β-blockade reduced non-fatal myocardial infarction (RR 0.73, p=0.001) but increased stroke (RR 1.73, p=0.05) and hypotension (RR 1.51, p<0.00001). These results were dominated by one large trial.
Conclusions: Guideline bodies should retract their recommendations based on fictitious data without further delay. This should not be blocked by dispute over allocation of blame. The well-conducted trials indicate a statistically significant 27% increase in mortality from the initiation of perioperative β-blockade that guidelines currently recommend. Any remaining enthusiasts might best channel their energy into a further randomised trial which should be designed carefully and conducted honestly.
Keywords: MYOCARDIAL ISCHAEMIA AND INFARCTION (IHD).
Figures


Comment in
- Heart. 2014 Mar;100(6):441-2
-
β-blockade to prevent perioperative death in non-cardiac surgery: questions, controversy, and not enough answers.Heart. 2014 Mar;100(6):443-4. doi: 10.1136/heartjnl-2013-305384. Heart. 2014. PMID: 24553256 No abstract available.
-
PURLs: Why you shouldn't start beta-blockers before surgery.J Fam Pract. 2014 Jun;63(6):E15-6. J Fam Pract. 2014. PMID: 25061626 Free PMC article.
References
-
- Task Force for Preoperative Cardiac Risk Assessment and Perioperative Cardiac Management in Non-cardiac Surgery, European Society of Cardiology (ESC); Poldermans D, Bax JJ, Boersma E, et al. Guidelines for pre-operative cardiac risk assessment and perioperative cardiac management in non-cardiac surgery: . Eur Heart J 2009;30:2769–812 - PubMed
-
- Poldermans D, Schouten O, Bax J, et al. Reducing cardiac risk in non-cardiac surgery: evidence from the DECREASE studies. Eur Heart J Suppl 2009; 11:A9–A14
-
- Erasmus Medical Centre Investigation into possible violation of scientific integrity. 2011. http://www.erasmusmc.nl/5663/135857/3664573/3397899/report_summary_inves... (accessed 10 Jul 2013)
-
- Erasmus Medical Centre Report on the 2012 follow-up investigation of possible breaches of academic integrity. 2012. http://cardiobrief.files.wordpress.com/2012/10/integrity-report-2012-10-... (accessed 10 Jul 2013)
-
- Poldermans D, Boersma E, Bax JJ, et al. The effect of bisoprolol on perioperative mortality and myocardial infarction in high-risk patients undergoing vascular surgery. Dutch Echocardiographic Cardiac Risk Evaluation Applying Stress Echocardiography Study Group. N Engl J Med 1999;341:1789–94 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous