

Allocating scarce resources in real-time to reduce heart failure readmissions: a prospective, controlled study
- PMID: 23904506
- PMCID: PMC3888600
- DOI: 10.1136/bmjqs-2013-001901
Allocating scarce resources in real-time to reduce heart failure readmissions: a prospective, controlled study
Abstract
Objective: To test a multidisciplinary approach to reduce heart failure (HF) readmissions that tailors the intensity of care transition intervention to the risk of the patient using a suite of electronic medical record (EMR)-enabled programmes.
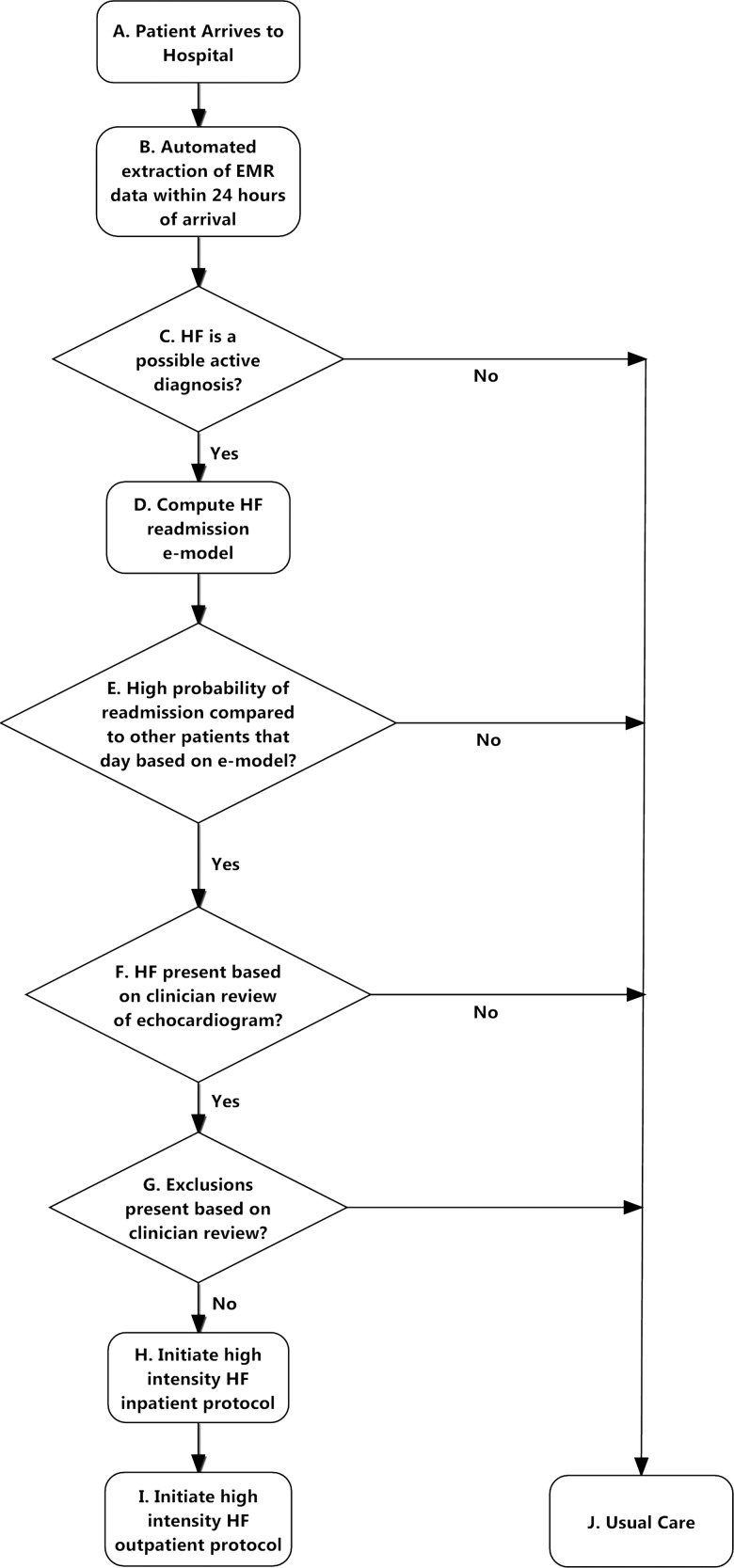
Methods: A prospective controlled before and after study of adult inpatients admitted with HF and two concurrent control conditions (acute myocardial infarction (AMI) and pneumonia (PNA)) was performed between 1 December 2008 and 1 December 2010 at a large urban public teaching hospital. An EMR-based software platform stratified all patients admitted with HF on a daily basis by their 30-day readmission risk using a published electronic predictive model. Patients at highest risk received an intensive set of evidence-based interventions designed to reduce readmission using existing resources. The main outcome measure was readmission for any cause and to any hospital within 30 days of discharge.
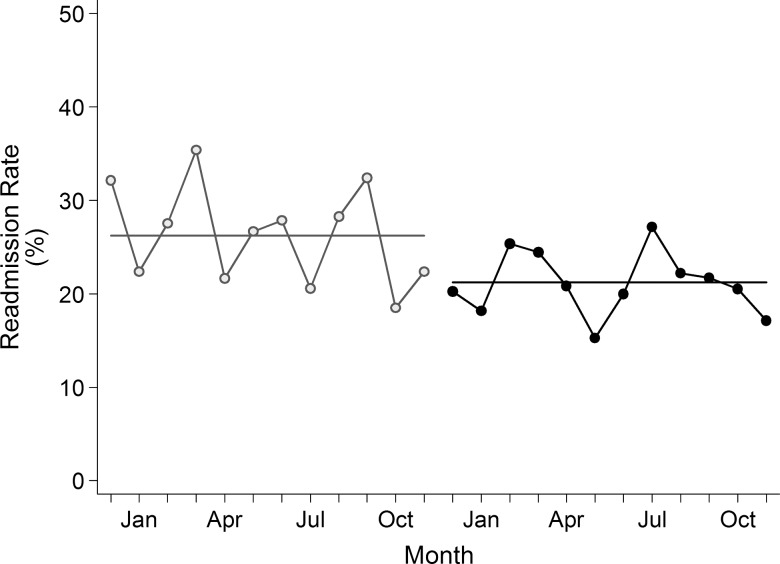
Results: There were 834 HF admissions in the pre-intervention period and 913 in the post-intervention period. The unadjusted readmission rate declined from 26.2% in the pre-intervention period to 21.2% in the post-intervention period (p=0.01), a decline that persisted in adjusted analyses (adjusted OR (AOR)=0.73; 95% CI 0.58 to 0.93, p=0.01). In contrast, there was no significant change in the unadjusted and adjusted readmission rates for PNA and AMI over the same period. There were 45 fewer readmissions with 913 patients enrolled and 228 patients receiving intervention, resulting in a number needed to treat (NNT) ratio of 20.
Conclusions: An EMR-enabled strategy that targeted scarce care transition resources to high-risk HF patients significantly reduced the risk-adjusted odds of readmission.
Keywords: Decision support, clinical; Health services research; Healthcare quality improvement; Information technology.
Figures
Comment in
-
Decreasing readmissions: it can be done but one size does not fit all.BMJ Qual Saf. 2013 Dec;22(12):975-6. doi: 10.1136/bmjqs-2013-002407. Epub 2013 Sep 4. BMJ Qual Saf. 2013. PMID: 24006457 No abstract available.
References
-
- Goodman DC, Fisher ES, Chang C-H. After hospitalization: a Dartmouth atlas report on post-acute care for Medicare beneficiaries. Hanover, NH: The Dartmouth Institute for Health Policy and Clinical Practice, 28 September 2011 - PubMed
-
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med 2009;360:1418–28 - PubMed
-
- Phillips CO, Wright SM, Kern DE, et al. Comprehensive discharge planning with postdischarge support for older patients with congestive heart failure. JAMA 2004;291:1358–67 - PubMed
-
- Seow H, Phillips CO, Rich MW, et al. Isolation of health services research from practice and policy: the example of chronic heart failure management. J Am Geriatr Soc 2006;54:535–40 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous