

Selective effects of baclofen on use-dependent modulation of GABAB inhibition after tetraplegia
- PMID: 23904624
- PMCID: PMC3728695
- DOI: 10.1523/JNEUROSCI.1552-13.2013
Selective effects of baclofen on use-dependent modulation of GABAB inhibition after tetraplegia
Abstract
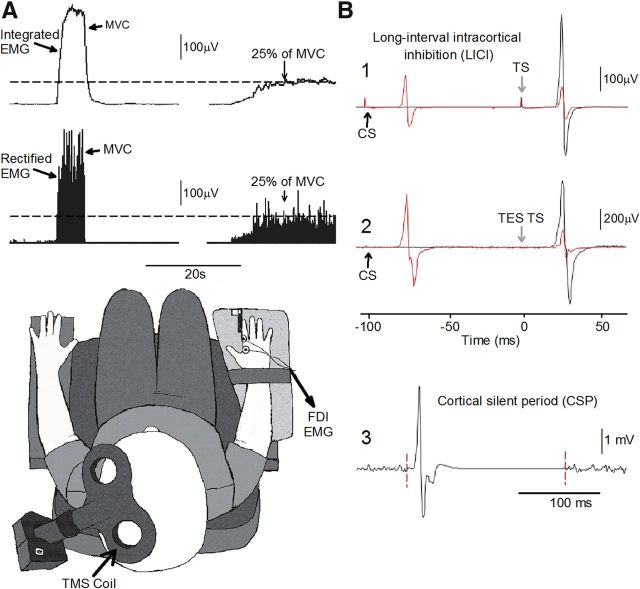
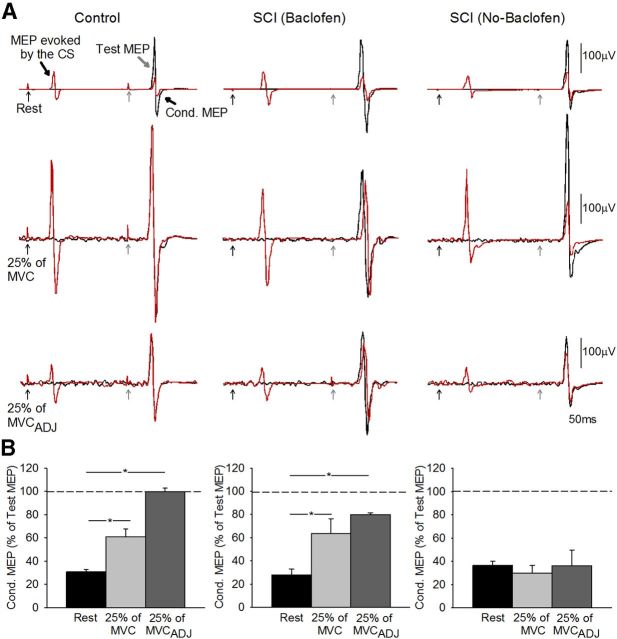
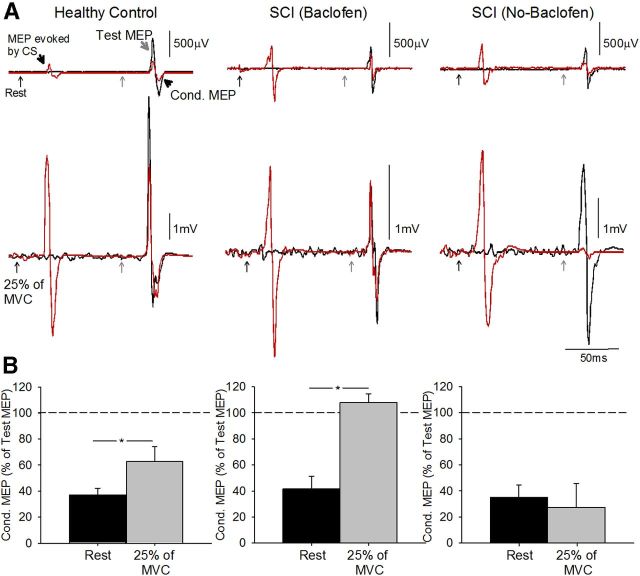
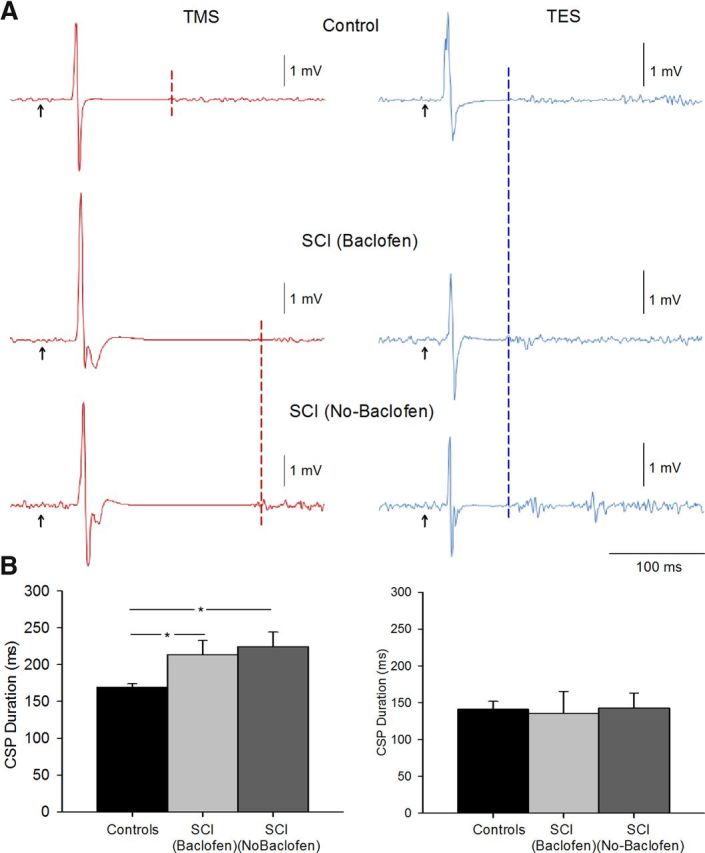
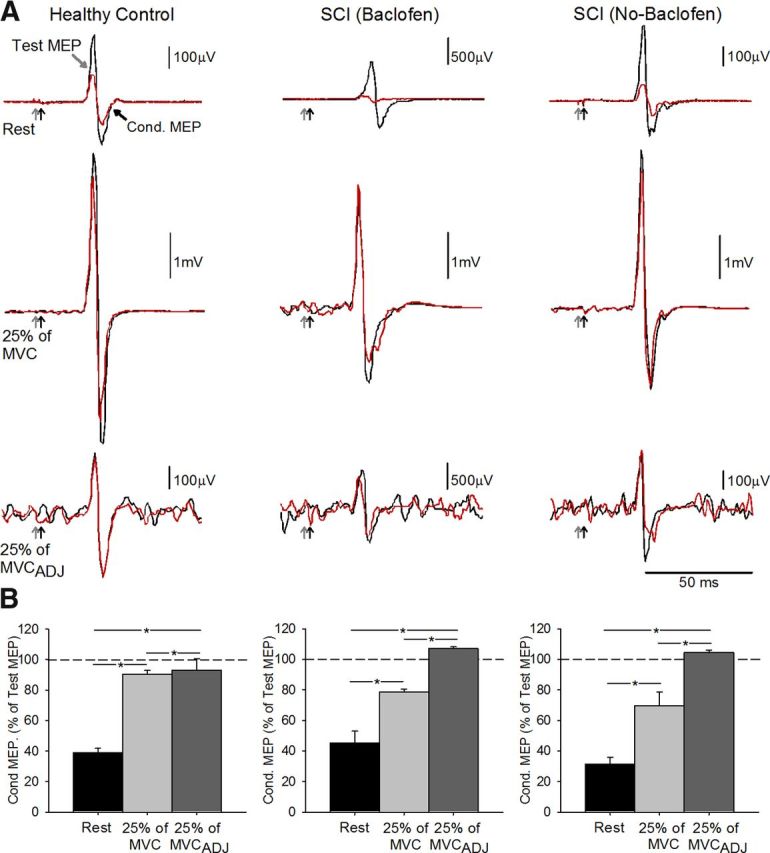
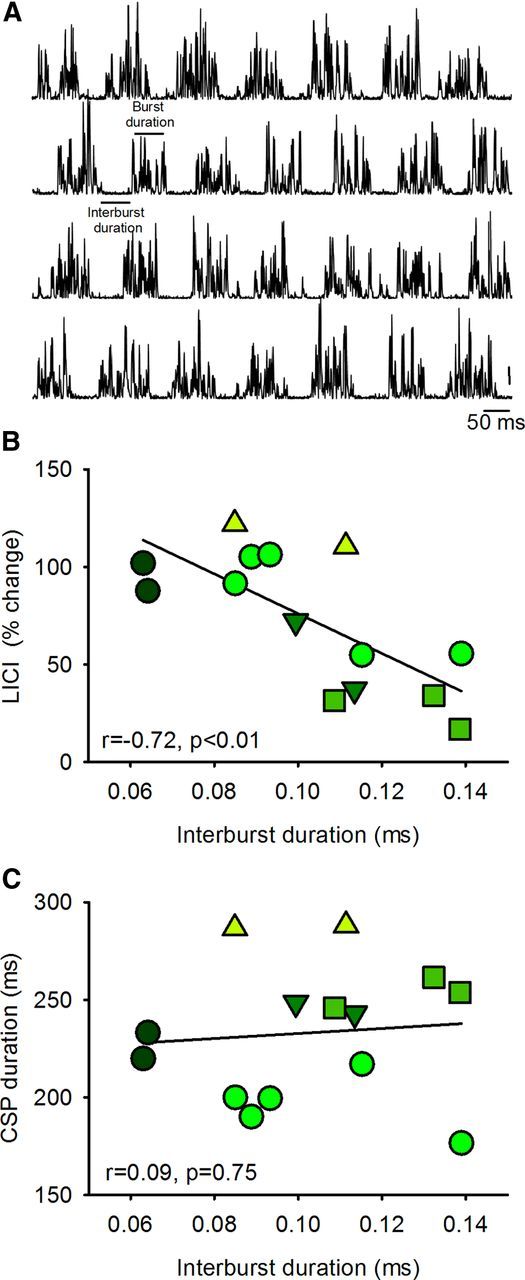
Baclofen is a GABAB receptor agonist commonly used to relief spasticity related to motor disorders. The effects of baclofen on voluntary motor output are limited and not yet understood. Using noninvasive transcranial magnetic and electrical stimulation techniques, we examined electrophysiological measures probably involving GABAB (long-interval intracortical inhibition and the cortical silent period) and GABAA (short-interval intracortical inhibition) receptors, which are inhibitory effects mediated by subcortical and cortical mechanisms. We demonstrate increased active long-interval intracortical inhibition and prolonged cortical silent period during voluntary activity of an intrinsic finger muscle in humans with chronic incomplete cervical spinal cord injury (SCI) compared with age-matched controls, whereas resting long-interval intracortical inhibition was unchanged. However, long-term (~6 years) use of baclofen decreased active long-interval intracortical inhibition to similar levels as controls but did not affect the duration of the cortical silent period. We found a correlation between signs of spasticity and long-interval intracortical inhibition in patients with SCI. Short-interval intracortical inhibition was decreased during voluntary contraction compared with rest but there was no effect of SCI or baclofen use. Together, these results demonstrate that baclofen selectively maintains use-dependent modulation of largely subcortical but not cortical GABAB neuronal pathways after human SCI. Thus, cortical GABA(B) circuits may be less sensitive to baclofen than spinal GABAB circuits. This may contribute to the limited effects of baclofen on voluntary motor output in subjects with motor disorders affected by spasticity.
Figures
References
-
- Beres-Jones JA, Johnson TD, Harkema SJ. Clonus after human spinal cord injury cannot be attributed solely to recurrent muscle-tendon stretch. Exp Brain Res. 2003;149:222–236. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources