

Antiphospholipid syndrome complicated by unilateral pleural effusion
- PMID: 23904846
- PMCID: PMC3728615
- DOI: 10.1159/000354135
Antiphospholipid syndrome complicated by unilateral pleural effusion
Abstract
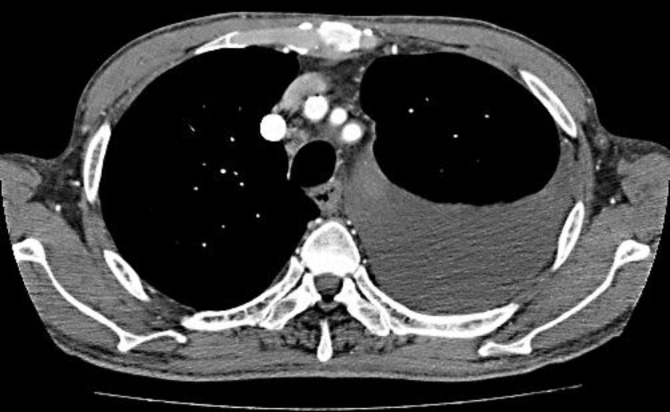
Antiphospholipid syndrome (APS) with pleural effusion is extremely rare. A 75-year-old man was admitted to our hospital for spreading erythema on his trunk and extremities, as well as dyspnea. One year before admission, he had visited us with a 1-year history of erythema and purpura on his legs and occasional fever. Given the diagnosis of APS, we initiated a combination therapy of aspirin and warfarin, but the skin lesions had gradually worsened. A biopsy specimen revealed marked thrombosis in the dermal and subcutaneous small vessels. In addition, chest X-ray and computed tomography demonstrated a large pleural effusion in the left lung. He underwent repeated drainage of the pleural effusion but the effusion recurred. We added oral prednisolone 30 mg daily to his prior anticoagulant therapy. The skin lesions and pleural effusion rapidly improved and disappeared without any complication. Corticosteroids might be a choice of treatment for intractable pleural effusion in APS patients.
Keywords: Antiphospholipid syndrome; Corticosteroids; Lupus-like disease; Pleural effusion.
Figures



References
-
- Vianna JL, Khamashta MA, Ordi-Ros J, et al. Comparison of the primary and secondary antiphospholipid syndrome: a European multicenter study of 114 patients. Am J Med. 1994;96:3–9. - PubMed
-
- Heffner JE, Brown LK, Barbieri CA. Diagnostic value of tests that discriminate between exudative and transudative pleural effusions. Primary Study Investigators. Chest. 1997;111:970–980. - PubMed
-
- Morita H, Daito H, Suwa T, et al. Overt congestive heart failure with mitral and aortic regurgitation due to antiphospholipid syndrome in a patient with systemic lupus erythematosus. Intern Med. 2000;39:506–511. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
