

Open reduction and internal fixation of unstable slipped capital femoral epiphysis by means of surgical dislocation does not decrease the rate of avascular necrosis: a preliminary study
- PMID: 23904893
- PMCID: PMC3425698
- DOI: 10.1007/s11832-012-0423-1
Open reduction and internal fixation of unstable slipped capital femoral epiphysis by means of surgical dislocation does not decrease the rate of avascular necrosis: a preliminary study
Abstract
Purpose: The treatment of unstable slipped capital femoral epiphysis (SCFE) remains controversial. Surgical dislocation and open reduction has the potential to significantly reduce the rate of avascular necrosis (AVN) by allowing direct preservation of the femoral head blood supply. The purpose of this study was to determine if open reduction of the unstable SCFE by means of surgical hip dislocation reduced the risk of AVN compared with closed reduction and percutaneous pinning.
Methods: We reviewed the medical records and radiographs of patients treated at our institution between the years 2000 and 2008. Sex, age, side of slip, precipitating event, pre- and post-operative anterior physeal separation (APS) and slip angle, slip severity, time between inciting event and surgical treatment, number of screws used, development of AVN, and need for subsequent surgery were evaluated. Statistical analysis was performed to compare risk factors and occurrence of AVN.
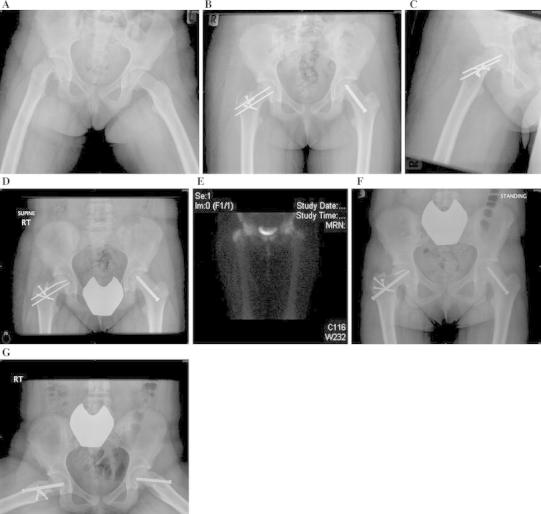
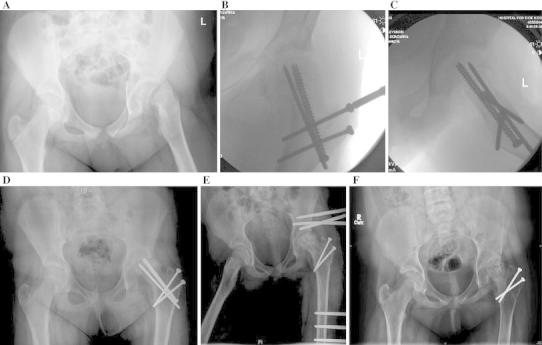
Results: From 2004 to 2008, we treated 12 patients with unstable SCFEs: six had closed reduction and percutaneous pinning and six underwent open reduction by means of surgical hip dislocation. There were no statistically significant differences between the two groups regarding sex, age, slip angle, APS, time to surgery, and AVN rate. At follow-up, 4 (66.7 %) patients had AVN in the group which had open reduction, while 2 (33.3 %) patients had AVN in the group which underwent closed reduction. (p = 0.57).
Conclusions: Open reduction of the unstable SCFE by means of surgical dislocation of the hip does not decrease the rate of AVN when compared to closed reduction.
Keywords: Avascular necrosis; Closed reduction; Open reduction; Percutaneous pinning; Slipped capital femoral epiphysis; Surgical dislocation of the hip.
Figures
Similar articles
-
Prevalence of Avascular Necrosis Following Surgical Treatments in Unstable Slipped Capital Femoral Epiphysis (SCFE): A Systematic Review and Meta-Analysis.Children (Basel). 2022 Sep 11;9(9):1374. doi: 10.3390/children9091374. Children (Basel). 2022. PMID: 36138683 Free PMC article. Review.
-
Purposeful Closed Reduction and Pinning in Unstable Slipped Capital Femoral Epiphysis Results in a Rate of Avascular Necrosis Comparable to the Literature Mean.Orthopedics. 2021 Mar-Apr;44(2):92-97. doi: 10.3928/01477447-20210201-02. Epub 2021 Feb 10. Orthopedics. 2021. PMID: 33561873
-
Outcome of in situ pinning in patients with unstable slipped capital femoral epiphysis: assessment of risk factors associated with avascular necrosis.J Pediatr Orthop. 2010 Jan-Feb;30(1):31-6. doi: 10.1097/BPO.0b013e3181c537b0. J Pediatr Orthop. 2010. PMID: 20032739
-
Outcome of the modified Dunn procedure in severe slipped capital femoral epiphysis.J Orthop Surg Res. 2020 Nov 3;15(1):506. doi: 10.1186/s13018-020-02036-3. J Orthop Surg Res. 2020. PMID: 33143737 Free PMC article.
-
What is the cause of avascular necrosis in unstable slipped capital femoral epiphysis and what can be done to lower the rate?J Pediatr Orthop. 2013 Jul-Aug;33 Suppl 1:S88-91. doi: 10.1097/BPO.0b013e318277172e. J Pediatr Orthop. 2013. PMID: 23764800 Review.
Cited by
-
A Retrospective Study of Risk Factors and Outcomes in the Surgical Management of Slipped Capital Femoral Epiphysis.J Am Acad Orthop Surg Glob Res Rev. 2022 Jul 6;6(7):e21.00135. doi: 10.5435/JAAOSGlobal-D-21-00135. eCollection 2022 Jul 1. J Am Acad Orthop Surg Glob Res Rev. 2022. PMID: 35794815 Free PMC article.
-
Idiopathic Slipped Capital Femoral Epiphysis: Demographic Differences and Similarities between Stable, Unstable, and Valgus Types.Children (Basel). 2023 Sep 15;10(9):1557. doi: 10.3390/children10091557. Children (Basel). 2023. PMID: 37761517 Free PMC article.
-
Mid-term outcomes of the modified Dunn procedure for slipped capital femoral epiphysis: results from a north African pediatric hip unit.J Orthop Surg Res. 2025 Jan 7;20(1):14. doi: 10.1186/s13018-024-05369-5. J Orthop Surg Res. 2025. PMID: 39773497 Free PMC article.
-
Prevalence of Avascular Necrosis Following Surgical Treatments in Unstable Slipped Capital Femoral Epiphysis (SCFE): A Systematic Review and Meta-Analysis.Children (Basel). 2022 Sep 11;9(9):1374. doi: 10.3390/children9091374. Children (Basel). 2022. PMID: 36138683 Free PMC article. Review.
-
Treatment of stable slipped capital femoral epiphysis: systematic review and exploratory patient level analysis.J Orthop Traumatol. 2017 Dec;18(4):379-394. doi: 10.1007/s10195-017-0469-4. Epub 2017 Aug 22. J Orthop Traumatol. 2017. PMID: 28831651 Free PMC article.
References
-
- Aronsson DD, Loder RT, Breur GJ, Weinstein SL. Slipped capital femoral epiphysis: current concepts. J Am Acad Orthop Surg. 2006;14(12):666–679. - PubMed
-
- Loder RT, Richards BS, Shapiro PS, Reznick LR, Aronson DD. Acute slipped capital femoral epiphysis: the importance of physeal stability. J Bone Joint Surg Am. 1993;75(8):1134–1140. - PubMed
-
- Aronsson DD, Loder RT. Treatment of the unstable (acute) slipped capital femoral epiphysis. Clin Orthop Relat Res. 1996;322:99–110. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
