

Association between daily antiretroviral pill burden and treatment adherence, hospitalisation risk, and other healthcare utilisation and costs in a US medicaid population with HIV
- PMID: 23906955
- PMCID: PMC3733306
- DOI: 10.1136/bmjopen-2013-003028
Association between daily antiretroviral pill burden and treatment adherence, hospitalisation risk, and other healthcare utilisation and costs in a US medicaid population with HIV
Abstract
Objectives: Lower pill burden leads to improved antiretroviral therapy (ART) adherence among HIV patients. Simpler dosing regimens have not been widely explored in real-world populations. We retrospectively assessed ART adherence, all-cause hospitalisation risk and costs, and other healthcare utilisation and costs in Medicaid enrollees with HIV treated with ART as a once-daily single-tablet regimen (STR) or two or more pills per day (2+PPD).
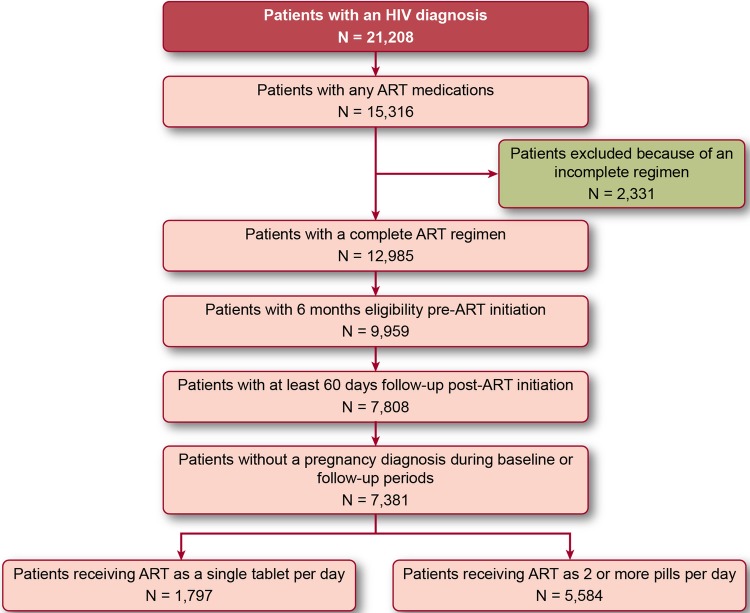
Design: Patients with an HIV diagnosis from 2005 to 2009 receiving complete ART (ie, two nucleoside/nucleotide reverse transcriptase inhibitors plus a third agent) for ≥60 days as STR or 2+PPD were selected and followed until the first of (1) discontinuation of the complete ART, (2) loss of enrolment or (3) end of database. Adherence was measured using the medication possession ratio. Monthly all-cause healthcare utilisation and costs were observed from regimen initiation until follow-up end.
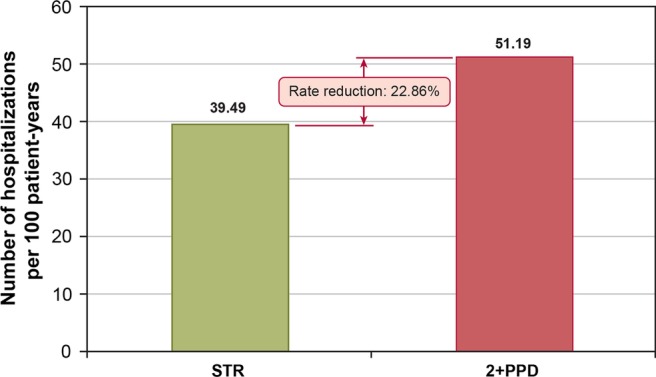
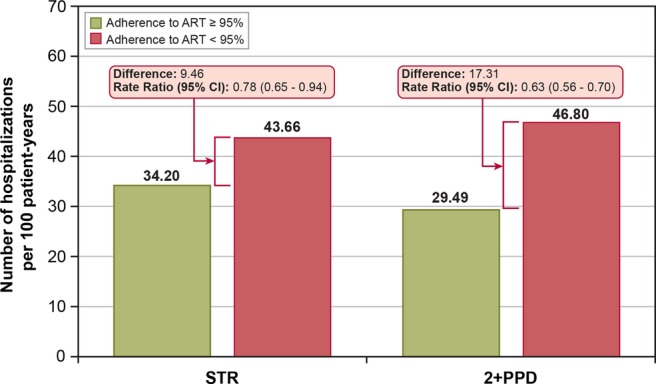
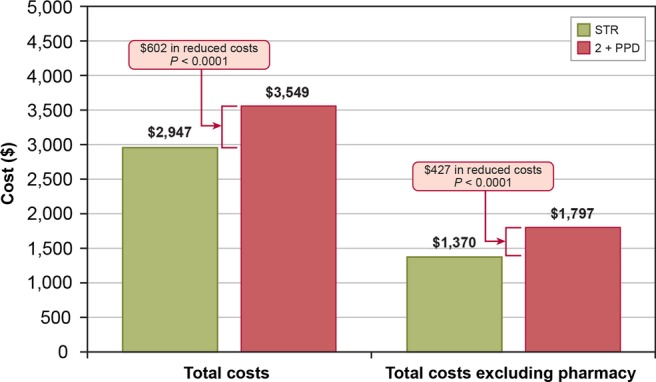
Results: Of the 7381 patients who met inclusion criteria, 1797 were treated with STR and 5584 with 2+PPD. STR patients were significantly more likely to reach 95% adherence and had fewer hospitalisations than 2+PPD patients (both p<0.01). STR patients had mean (SD) total monthly costs of $2959 ($4962); 2+PPD patients had $3544 ($5811; p<0.001). Hospital costs accounted for 53.8% and pharmacy costs accounted for 32.5% of this difference. Multivariate analyses found that STR led to a 23% reduction in hospitalisations and a 17% reduction in overall healthcare costs. ART adherence appears to be a key mechanism mediating hospitalisation risk, as patients with ≥95% adherence (regardless of regimen type) had a lower hospitalisation rate compared with <95% adherence.
Conclusions: While it was expected that STR patients would have lower pharmacy costs, we also found that STR patients had fewer hospitalisations and lower hospital costs than 2+PPD patients, resulting in significantly lower total healthcare costs for STR patients.
Keywords: Health Economics; Therapeutics.
Figures
References
-
- Thompson MA, Aberg JA, Cahn P, et al. Recommendations of the IAS-USA Panel. JAMA 2010;304:321–33 - PubMed
-
- Henry K. Report from the 17th Conference on Retroviruses and Opportunistic Infections. More data and answers from ACTG 5202. J Watch AIDS Clin Care 2010;22:30. - PubMed
-
- Rockstroh JK, Lennox JL, Dejesus E, et al. STARTMRK Investigators Long-term treatment with raltegravir or efavirenz combined with tenofovir/emtricitabine for treatment-naïve human immunodeficiency virus-1-infected patients: 156-week results from STARTMRK. Clin Infect Dis 2011;53:807–16 - PubMed
-
- Fielden SJ, Rusch ML, Yip B, et al. Nonadherence increases the risk of hospitalization among HIV-infected antiretroviral naïve patients started on HAART. J Int Assoc Phys AIDS Care 2008;7:238–44 - PubMed
-
- Kitahata MM, Reed SD, Dillingham PW, et al. Pharmacy-based assessment of adherence to HAART predicts virological and immunologic treatment response and clinical progression to AIDS and death. Int J STD AIDS 2004;15:803–10 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous