

Identifying future 'unexpected' survivors: a retrospective cohort study of fatal injury patterns in victims of improvised explosive devices
- PMID: 23906957
- PMCID: PMC3733302
- DOI: 10.1136/bmjopen-2013-003130
Identifying future 'unexpected' survivors: a retrospective cohort study of fatal injury patterns in victims of improvised explosive devices
Abstract
Objectives: To identify potentially fatal injury patterns in explosive blast fatalities in order to focus research and mitigation strategies, to further improve survival rates from blast trauma.
Design: Retrospective cohort study.
Participants: UK military personnel killed by improvised explosive device (IED) blasts in Afghanistan, November 2007-August 2010.
Setting: UK military deployment, through NATO, in support of the International Security Assistance Force (ISAF) mission in Afghanistan.
Data sources: UK military postmortem CT records, UK Joint Theatre Trauma Registry and associated incident data.
Main outcome measures: Potentially fatal injuries attributable to IEDs.
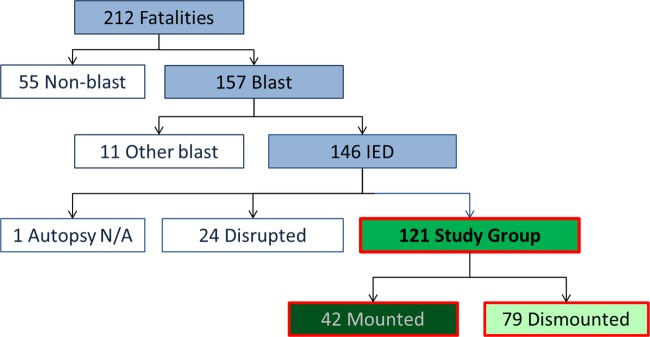
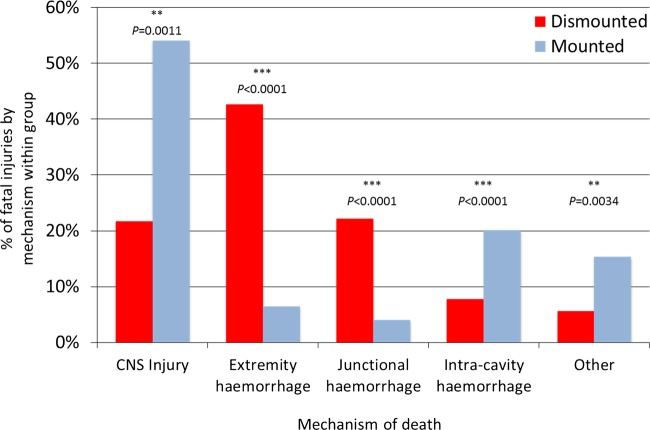
Results: We identified 121 cases, 42 mounted (in-vehicle) and 79 dismounted (on foot), at a point of wounding. There were 354 potentially fatal injuries in total. Leading causes of death were traumatic brain injury (50%, 62/124 fatal injuries), followed by intracavity haemorrhage (20.2%, 25/124) in the mounted group, and extremity haemorrhage (42.6%, 98/230 fatal injuries), junctional haemorrhage (22.2%, 51/230 fatal injuries) and traumatic brain injury (18.7%, 43/230 fatal injuries) in the dismounted group.
Conclusions: Head trauma severity in both mounted and dismounted IED fatalities indicated prevention and mitigation as the most effective strategies to decrease resultant mortality. Two-thirds of dismounted fatalities had haemorrhage implicated as a cause of death that may have been anatomically amenable to prehospital intervention. One-fifth of the mounted fatalities had haemorrhagic trauma which currently could only be addressed surgically. Maintaining the drive to improve all haemostatic techniques for blast casualties, from point of wounding to definitive surgical proximal vascular control, alongside the development and application of novel haemostatic interventions could yield a significant survival benefit. Prospective studies in this field are indicated.
Keywords: Battlefield Trauma; Cause of Death; IED.
Figures
References
-
- icasualties.org online casualty database. http://icasualties.org/OEF/Fatalities.aspx (accessed 11 Jun 2012).
-
- Shelton HH. Pub 3-07.2 Joint tactics, techniques, and procedures for antiterrorism. Washington: Department of Defense, 1998
-
- Ramasamy A, Hill AM, Clasper JC. Improvised explosive devices: pathophysiology, injury profiles and current medical management. J R Army Med Corps 2009;155:265–72 - PubMed
-
- Bosker AJ. IEDs will remain ‘weapon of choice’ for decades. Joint Improvised Explosive Device Defeat Organisation (JIEDDO), US Department of Defense 21 September 2012. https://www.jieddo.mil/news_story.aspx?ID=1488 (accessed 15 Dec 2012).
-
- Mazurek MT, Ficke JR. The scope of wounds encountered in casualties from the global war on terrorism: from the battlefield to the tertiary treatment facility. J Am Acad Orthop Surg 2006;14:S18–23 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials