

Imaging recommendations for acute stroke and transient ischemic attack patients: A joint statement by the American Society of Neuroradiology, the American College of Radiology, and the Society of NeuroInterventional Surgery
- PMID: 23907247
- PMCID: PMC4072500
- DOI: 10.3174/ajnr.A3690
Imaging recommendations for acute stroke and transient ischemic attack patients: A joint statement by the American Society of Neuroradiology, the American College of Radiology, and the Society of NeuroInterventional Surgery
Abstract
Stroke is a leading cause of death and disability worldwide. Imaging plays a critical role in evaluating patients suspected of acute stroke and transient ischemic attack, especially before initiating treatment. Over the past few decades, major advances have occurred in stroke imaging and treatment, including Food and Drug Administration approval of recanalization therapies for the treatment of acute ischemic stroke. A wide variety of imaging techniques has become available to assess vascular lesions and brain tissue status in acute stroke patients. However, the practical challenge for physicians is to understand the multiple facets of these imaging techniques, including which imaging techniques to implement and how to optimally use them, given available resources at their local institution. Important considerations include constraints of time, cost, access to imaging modalities, preferences of treating physicians, availability of expertise, and availability of endovascular therapy. The choice of which imaging techniques to employ is impacted by both the time urgency for evaluation of patients and the complexity of the literature on acute stroke imaging. Ideally, imaging algorithms should incorporate techniques that provide optimal benefit for improved patient outcomes without delaying treatment.
Figures
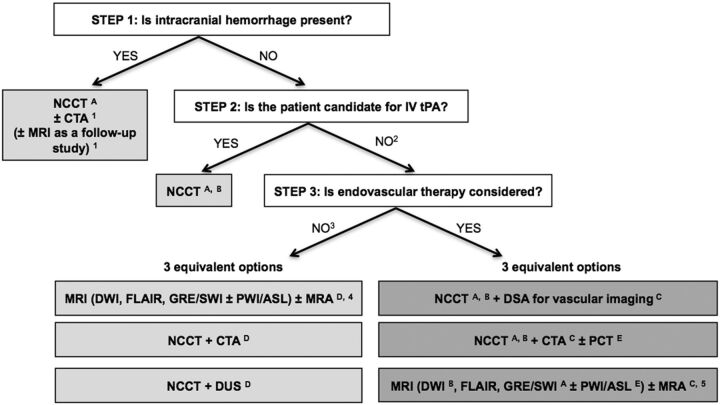
To assess the etiology of the intracranial hemorrhage (CTA for vascular pathologies, such as aneurysms, arteriovenous malformations, vasculopathies; MR imaging for vascular malformations, neoplastic and other pathologies associated with hemorrhage).
Also if the patient is not a candidate for IV tPA (contraindication to tPA, outside the time window for tPA) or if IV tPA failed or it is thought that it may fail.
For patients who are outside the time window for acute reperfusion therapies (>4.5 hours at sites where only IV tPA is being considered; >8 hours at sites where endovascular therapy is considered) and for patients with TIAs, emphasis is on secondary prevention and their imaging work-up should be focused on vascular imaging (CTA, MRA or Doppler-ultrasound [DUS]) to assess carotid arteries as a possible cause of the ischemic stroke, with secondary prevention in mind. If MRA is obtained, it makes sense to concurrently obtain MR imaging with DWI, FLAIR, and GRE/SWI. Echocardiography should also be obtained to assess for cardiac sources.
If available, MR imaging/MRA is the preferred imaging technique for TIA patients.
At institutions where MR imaging is available 24/7 and can be performed within a short time after admission.
To assess for intracranial hemorrhage.
To assess the extent of ischemic core.
To assess the location and extent of the intravascular clot.
To assess carotid atherosclerotic disease.
To assess the extent of viable tissue.
Comment in
-
Stroke imaging: diffusion, perfusion, but no more confusion!AJNR Am J Neuroradiol. 2013 Nov-Dec;34(11):2053. doi: 10.3174/ajnr.A3691. Epub 2013 Aug 1. AJNR Am J Neuroradiol. 2013. PMID: 23907248 Free PMC article. No abstract available.
References
-
- Rowley HA. Extending the time window for thrombolysis: evidence from acute stroke trials. Neuroimaging Clin N Am 2005;15:575–87, x - PubMed
-
- Sims J, Schwamm LH. The evolving role of acute stroke imaging in intravenous thrombolytic therapy: patient selection and outcomes assessment. Neuroimaging Clin N Am 2005;15:421–40, xii - PubMed
-
- Schellinger PD. The evolving role of advanced MR imaging as a management tool for adult ischemic stroke: a Western-European perspective. Neuroimaging Clin N Am 2005;15:245–58, ix - PubMed
-
- Oxford University. Oxford Centre for Evidence-based Medicine - Levels of Evidence (March 2009) http://www.cebm.net/?O=1025 Accessed June 26, 2013.
-
- DeLaPaz RL, Wippold FJ, 2nd, Cornrlius RS, et al. ACR appropriateness criteria® on cerebrovascular disease. J Am Coll Radiol 2011;8:532–38 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous