

The PRESERVE mortality risk score and analysis of long-term outcomes after extracorporeal membrane oxygenation for severe acute respiratory distress syndrome
- PMID: 23907497
- PMCID: PMC7094902
- DOI: 10.1007/s00134-013-3037-2
The PRESERVE mortality risk score and analysis of long-term outcomes after extracorporeal membrane oxygenation for severe acute respiratory distress syndrome
Abstract
Purpose: This study was designed to identify factors associated with death by 6 months post-intensive care unit (ICU) discharge and to develop a practical mortality risk score for extracorporeal membrane oxygenation (ECMO)-treated acute respiratory distress syndrome (ARDS) patients. We also assessed long-term survivors' health-related quality of life (HRQL), respiratory symptoms, and anxiety, depression and post-traumatic stress disorder (PTSD) frequencies.
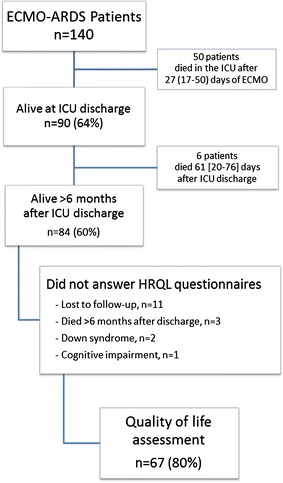
Methods: Data from 140 ECMO-treated ARDS patients admitted to three French ICUs (2008-2012) were analyzed. ICU survivors contacted >6 months post-ICU discharge were assessed for HRQL, psychological and PTSD status.
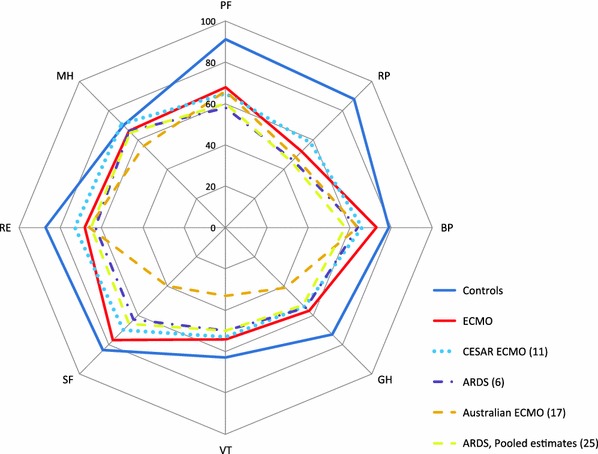
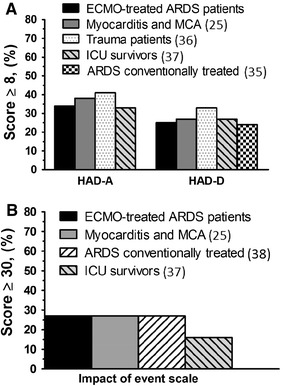
Results: Main ARDS etiologies were bacterial (45%), influenza A[H₁N₁] (26%) and post-operative (17%) pneumonias. Six months post-ICU discharge, 84 (60%) patients were still alive. Based on multivariable logistic regression analysis, the PRESERVE (PRedicting dEath for SEvere ARDS on VV-ECMO) score (0-14 points) was constructed with eight pre-ECMO parameters, i.e. age, body mass index, immunocompromised status, prone positioning, days of mechanical ventilation, sepsis-related organ failure assessment, plateau pressure andpositive end-expiratory pressure. Six-month post-ECMO initiation cumulative probabilities of survival were 97, 79, 54 and 16% for PRESERVE classes 0-2, 3-4, 5-6 and ≥7 (p < 0.001), respectively. HRQL evaluation in 80% of the 6-month survivors revealed satisfactory mental health but persistent physical and emotional-related difficulties, with anxiety, depression or PTSD symptoms reported, by 34, 25 or 16%, respectively.
Conclusions: The PRESERVE score might help ICU physicians select appropriate candidates for ECMO among severe ARDS patients. Future studies should also focus on physical and psychosocial rehabilitation that could lead to improved HRQL in this population.
Trial registration: ClinicalTrials.gov NCT01470703.
Figures

Comment in
-
Outcomes and risk stratification for severe ARDS treated with ECMO.Intensive Care Med. 2013 Oct;39(10):1857-60. doi: 10.1007/s00134-013-3067-9. Epub 2013 Aug 17. Intensive Care Med. 2013. PMID: 23955556 No abstract available.
-
Influence of ventilatory strategy on the PRESERVE mortality risk score.Intensive Care Med. 2014 Feb;40(2):296. doi: 10.1007/s00134-013-3168-5. Epub 2013 Dec 4. Intensive Care Med. 2014. PMID: 24306081 No abstract available.
References
-
- Sud S, Friedrich JO, Taccone P, Polli F, Adhikari NK, Latini R, Pesenti A, Guerin C, Mancebo J, Curley MA, Fernandez R, Chan MC, Beuret P, Voggenreiter G, Sud M, Tognoni G, Gattinoni L. Prone ventilation reduces mortality in patients with acute respiratory failure and severe hypoxemia: systematic review and meta-analysis. Intensive Care Med. 2010;36:585–599. doi: 10.1007/s00134-009-1748-1. - DOI - PubMed
-
- Herridge MS, Cheung AM, Tansey CM, Matte-Martyn A, Diaz-Granados N, Al-Saidi F, Cooper AB, Guest CB, Mazer CD, Mehta S, Stewart TE, Barr A, Cook D, Slutsky AS. One-year outcomes in survivors of the acute respiratory distress syndrome. N Engl J Med. 2003;348:683–693. doi: 10.1056/NEJMoa022450. - DOI - PubMed
-
- Herridge MS, Tansey CM, Matte A, Tomlinson G, Diaz-Granados N, Cooper A, Guest CB, Mazer CD, Mehta S, Stewart TE, Kudlow P, Cook D, Slutsky AS, Cheung AM. Functional disability 5 years after acute respiratory distress syndrome. N Engl J Med. 2011;364:1293–1304. doi: 10.1056/NEJMoa1011802. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
