

Skeletal involvement in Langerhans cell histiocytosis
- PMID: 23907805
- PMCID: PMC3781243
- DOI: 10.1007/s13244-013-0271-7
Skeletal involvement in Langerhans cell histiocytosis
Abstract
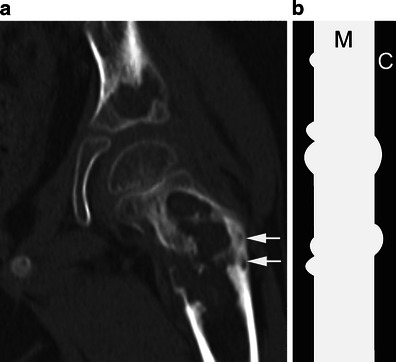
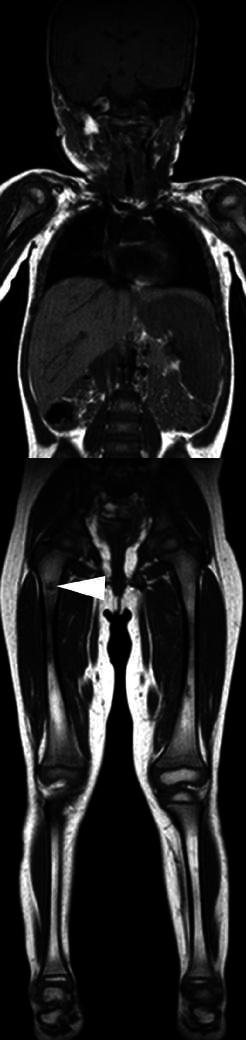
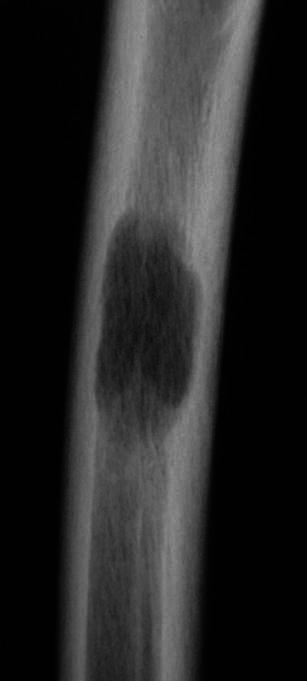
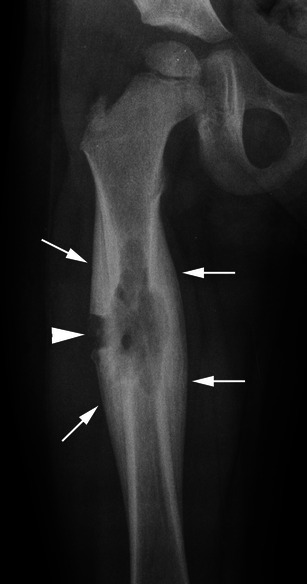
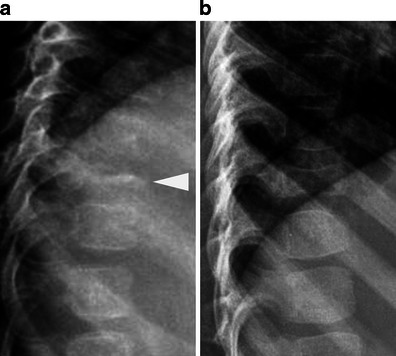
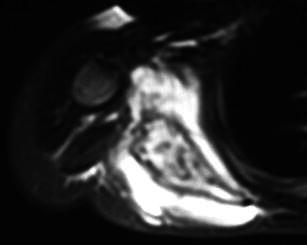
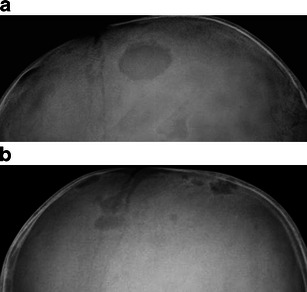
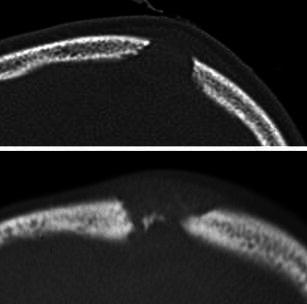
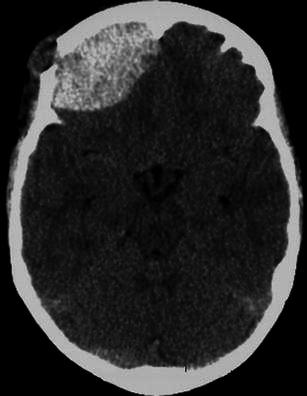
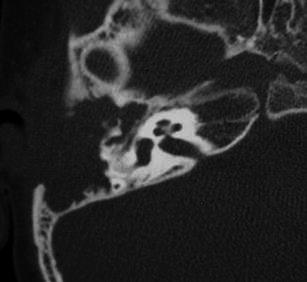
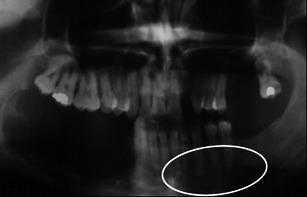
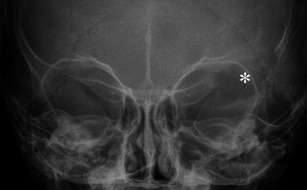
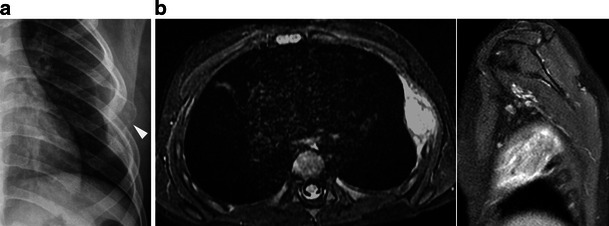
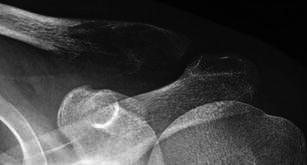
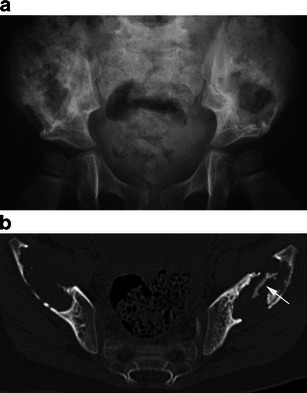
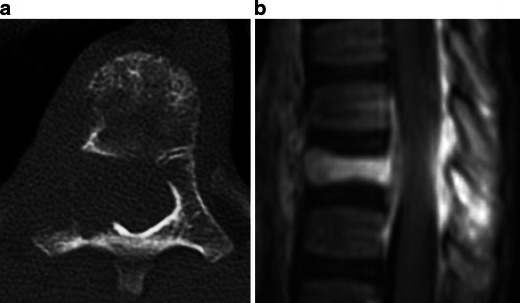
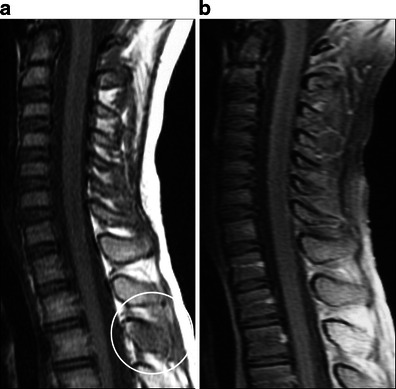
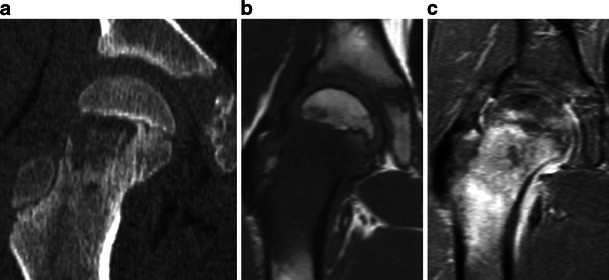
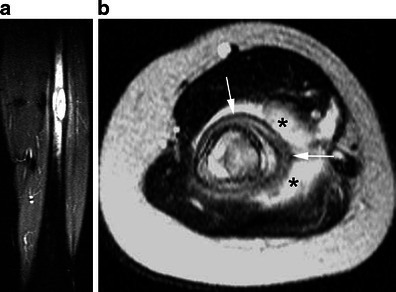
Langerhans cell histiocytosis (LCH) represents a disorder characterised by an abnormal accumulation of histiocytes in miscellaneous tissues. The bone is commonly affected, especially the flat bones, the spine and the long bones. Some lesions in children such as a "vertebra plana" or a solitary lytic lesion of the skull may be suggestive for LCH, whereas others can be confused with a malignant tumour or osteomyelitis. This pictorial essay presents the main usual and unusual skeletal manifestations observed in LCH.
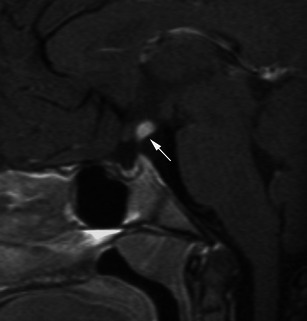
Teaching points: • Osseous involvement in children with LCH is very similar to that seen in multiple myeloma. • A solitary lytic lesion of the cranial vault is a typical radiographic finding of LCH. • A vertebra plana appearance in the spine is another typical radiographic finding. • Extensive signal intensity changes within bone marrow on MRI are a helpful sign for the diagnosis. • In long bones, endosteal scalloping may be responsible for a "budding appearance".
Figures



References
-
- Leonidas JC, Guelfguat M, Valderrama E. Langerhans’ cell histiocytosis (203) Lancet 361:1293–1295 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
