

Review
doi: 10.1259/bjr.20130284.
Epub 2013 Aug 1.
Venous compression syndromes: clinical features, imaging findings and management
Affiliations
- PMID: 23908347
- PMCID: PMC3798333
- DOI: 10.1259/bjr.20130284
Item in Clipboard
Review
Venous compression syndromes: clinical features, imaging findings and management
Br J Radiol.
2013 Oct.
Abstract
Extrinsic venous compression is caused by compression of the veins in tight anatomic spaces by adjacent structures, and is seen in a number of locations. Venous compression syndromes, including Paget-Schroetter syndrome, Nutcracker syndrome, May-Thurner syndrome and popliteal venous compression will be discussed. These syndromes are usually seen in young, otherwise healthy individuals, and can lead to significant overall morbidity. Aside from clinical findings and physical examination, diagnosis can be made with ultrasound, CT, or MR conventional venography. Symptoms and haemodynamic significance of the compression determine the ideal treatment method.
Figures
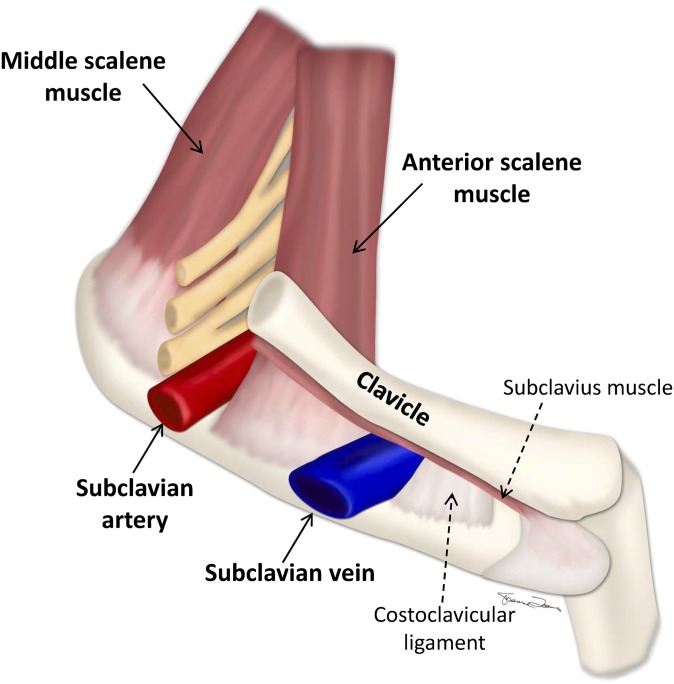
Interscalene triangle and the costoclavicular space. The subclavian vein can be seen coursing through the costoclavicular space, bordered by the clavicle superiorly, the first rib inferiorly and the anterior scalene muscle posteriorly. The relationship of the costoclavicular space to the interscalene triangle through which the subclavian artery and the brachial plexus travels can also be seen.
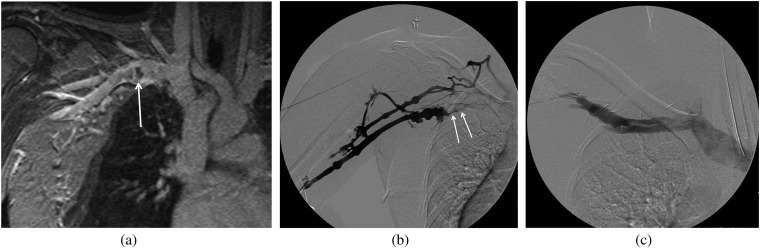
A 27-year-old female athlete presenting with right arm swelling. Initial ultrasound showed deep venous thrombosis in the subclavian vein. (a) Coronal MR venography demonstrates focal thrombus (arrow) in the subclavian vein with focal dilatation and surrounding collaterals in the chest wall. (b) Right upper extremity venogram was performed showing acute thrombus (arrows), luminal irregularity and collaterals surrounding the subclavian vein that was treated with catheter-directed thrombolysis. (c) Repeat venogram following first rib resection shows resolution of the findings.

A 25-year-old female who presented with pelvic pain and was also found to have haematuria. (a–c) A contrast-enhanced CT scan was performed to evaluate the cause of pain. An axial scan at the level of (a) the left renal vein (LRV) and (b) in the pelvis, and (c) a coronal scan through the gonadal vein demonstrate compression of the LRV (arrow) by the superior mesenteric artery anteriorly and the aorta posteriorly, multiple pelvic collateral vessels and an enlarged gonadal vein. (d–e) The patient later underwent a venogram to demonstrate the reflux and to coil embolise the gonadal vein. (d) Venogram via a right common femoral vein access and injection of the gonadal vein demonstrates an enlarged gonadal vein and cross pelvic collaterals with partial opacification of the right gonadal vein. (e) Venogram following coil embolisation of the left gonadal vein shows absence of reflux.
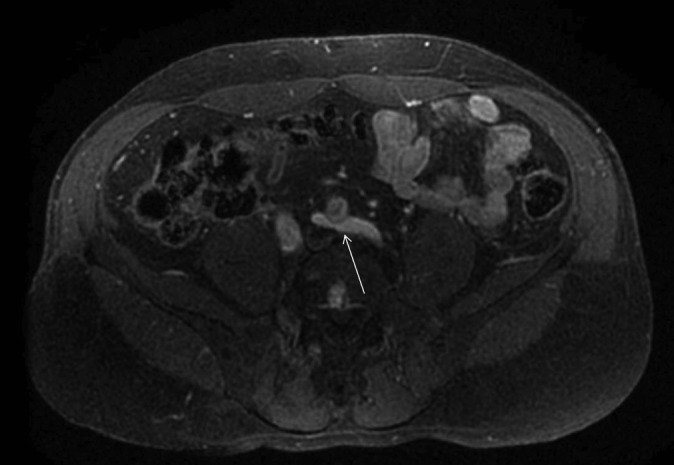
A 38-year-old female with pelvic pain and left lower extremity swelling. MR venography (MRV) was obtained to evaluate for May–Thurner syndrome (MTS). Axial image from the contrast-enhanced MRV demonstrates a variation of MTS, with compression of the left iliac vein (arrow) by the left common iliac artery.
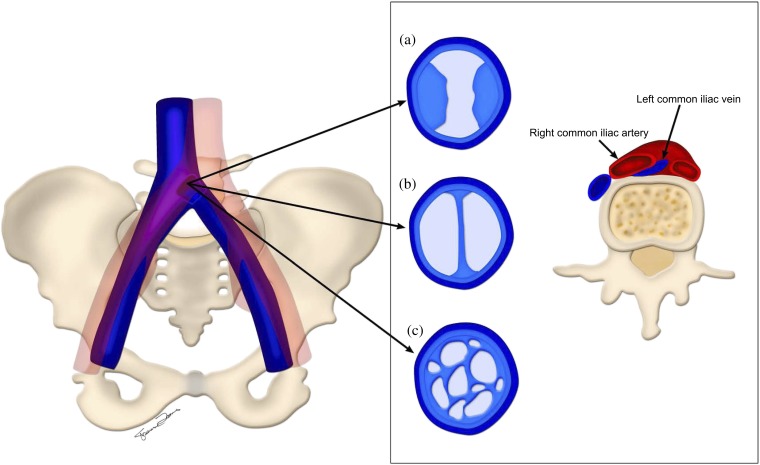
Left common iliac vein compression by the right common iliac artery. Chronic changes in the left common iliac vein secondary to endothelial damage with (a) intraluminal spurs, (b) webs and (c) channels are depicted.
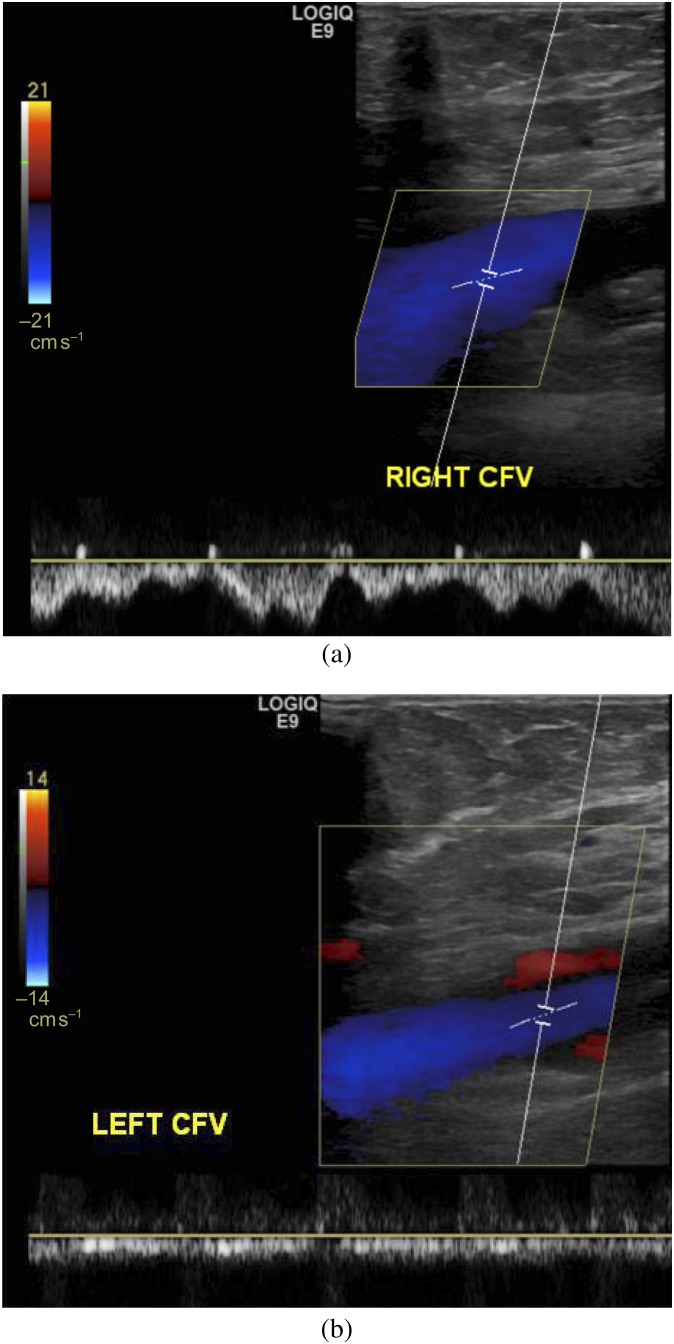
A 28-year-old female with left lower extremity swelling and varices. (a, b) Doppler ultrasound was performed to evaluate for deep venous thrombosis. (a) Right common femoral vein shows normal respiratory variation. (b) Left common femoral vein (CFV) study shows the absence of normal respiratory variation, suggesting more central (left iliac vein) obstruction. This patient was later found to have May–Thurner syndrome.
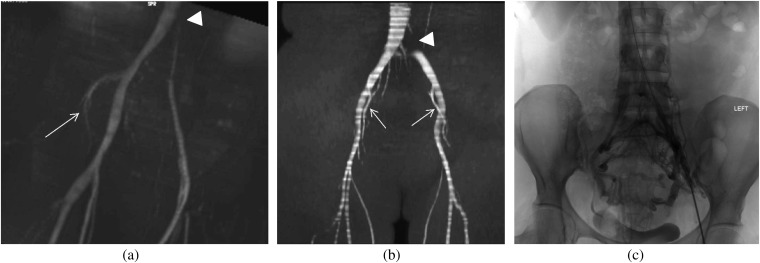
A 33-year-old female with unilateral, left-sided lower extremity pain, swelling and heaviness as well as chronic pelvic pain. (a) Coronal maximum intensity projection from the time of flight sequence of the MR venography obtained to further evaluate the cause of her symptoms demonstrates compression of the left common iliac vein which is diminished in calibre with a focal signal void (arrowhead). The left internal iliac vein is not visualised consistent with retrograde flow, which suggests haemodynamically significant left common iliac venous compression. However, the right internal iliac vein is seen (arrow). (b) The same sequence in another patient given for comparison purposes shows a focal signal void in the left common iliac artery at the point of compression (arrowhead), but a signal is seen in the internal iliac arteries (arrows), suggesting antigrade direction of flow. (c) The patient underwent a venogram for further evaluation and possible stenting, which shows some luminal irregularity of the left common iliac vein with multiple pelvic collaterals.
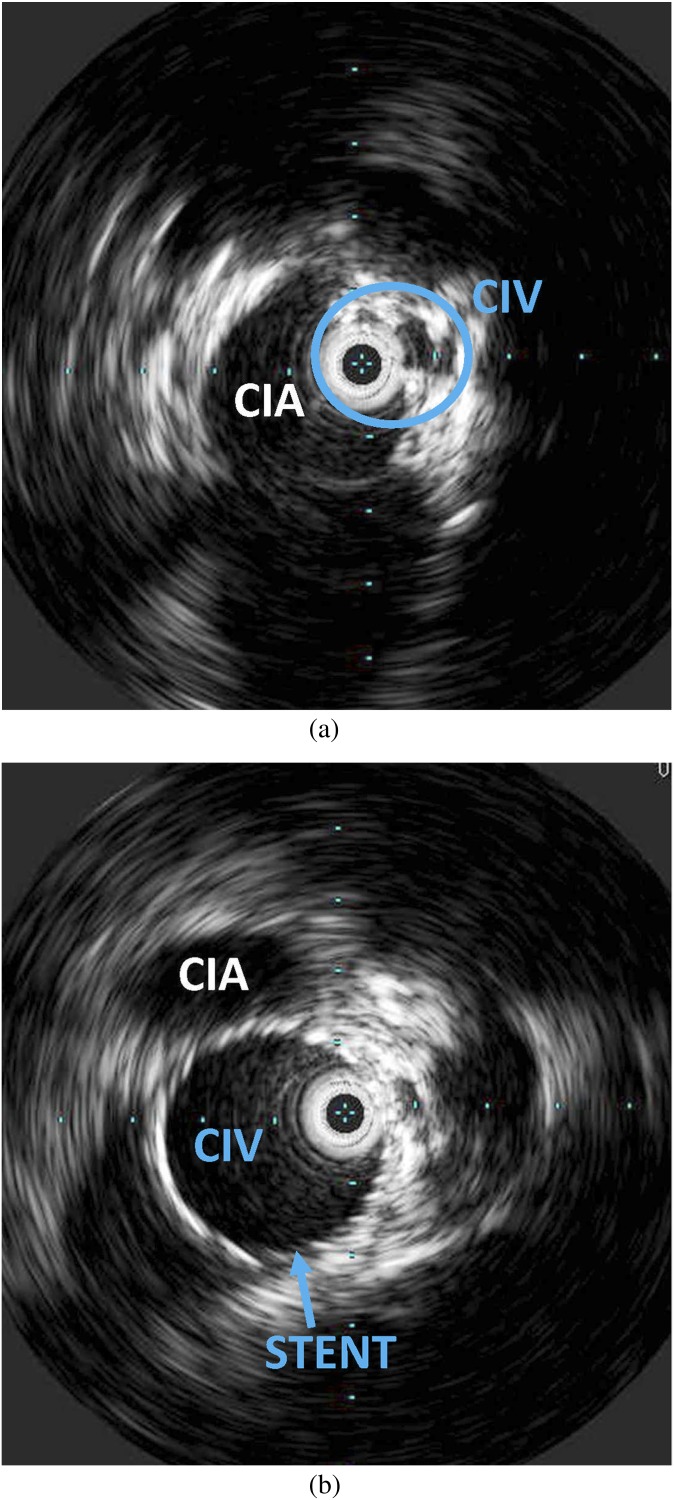
A 32-year-old female with an established diagnosis of May–Thurner syndrome. Patient has had recurrent episodes of unilateral deep venous thrombosis and swelling in the left lower extremity. (a, b) Intravascular ultrasound was performed before and after stenting of the left common iliac vein (CIV) to relieve the compression. (a) Wall thickening and intraluminal irregularity of the left CIV and extrinsic compression by the adjacent right common iliac artery (CIA) are seen obtained prior to stenting. The intravascular ultrasound probe can be seen in the encircled CIV. (b) Following stenting, the lumen is widely patent.
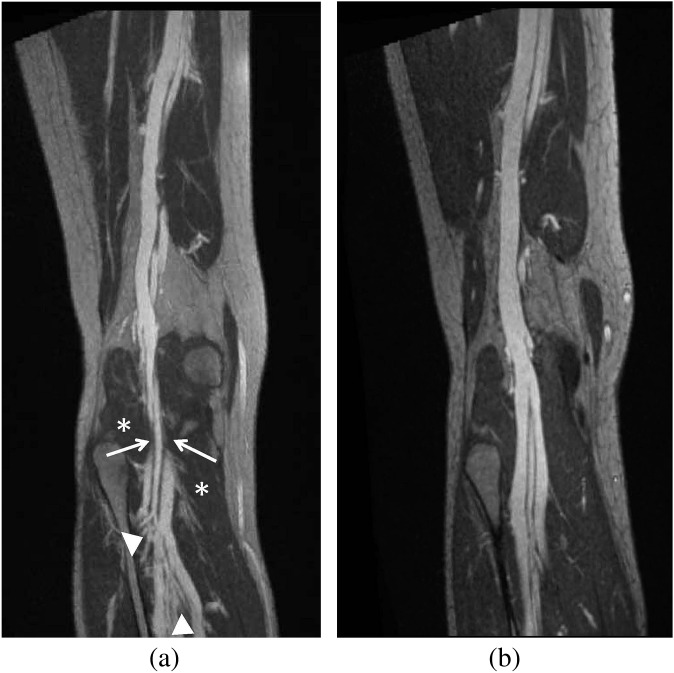
A 32-year-old female with right lower extremity, below the knee swelling, varicosities and venous ulceration at the medial malleolus. (a, b) Three-dimensional-curved maximum intensity projection coronal images from a high-resolution MR venography study using gadofoveset trisodium. (a) Pre-operative image shows popliteal venous compression (arrow) at the level of the popliteal fossa with multiple varices (arrowheads) below the point of compression. The gastrocnemius muscle is seen (*). (b) Post-operative image obtained at the same level following surgical release of the medial head of the gastrocnemius muscle shows resolution of the compression.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
