

MRI-Guided Electrophysiology Intervention
- PMID: 23908787
- PMCID: PMC3678784
- DOI: 10.5041/RMMJ.10015
MRI-Guided Electrophysiology Intervention
Erratum in
-
Correction for the Article "MRI-Guided Electrophysiology Intervention" by Henry R. Halperin and Aravindan Kolandaivelu.Rambam Maimonides Med J. 2015 Jul 30;6(3):e0036. doi: 10.5041/RMMJ.10206. Rambam Maimonides Med J. 2015. PMID: 26241227 Free PMC article. No abstract available.
Abstract
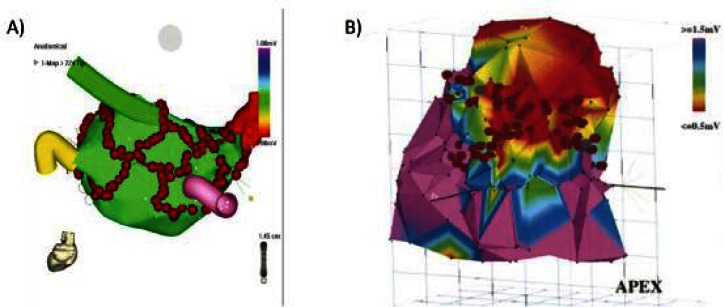
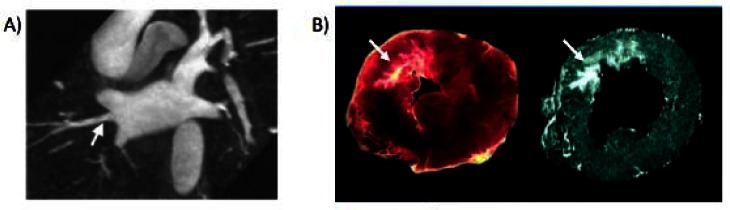
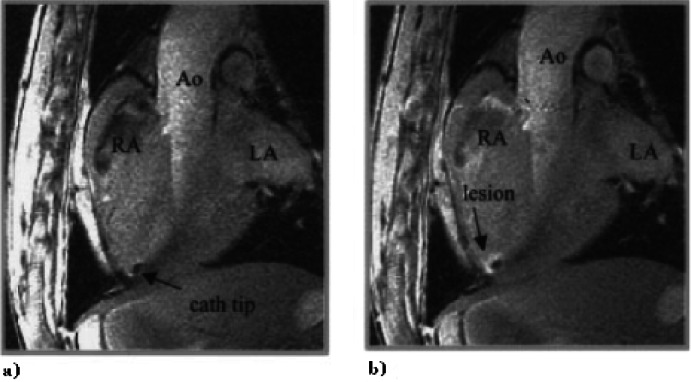
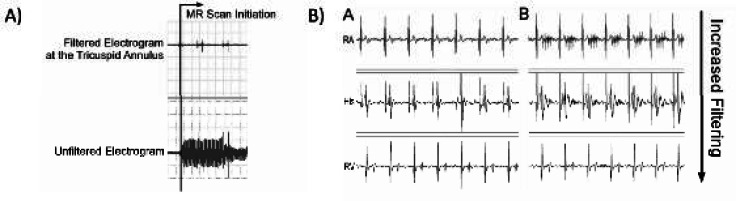
Catheter ablation is a first-line treatment for many cardiac arrhythmias and is generally performed under X-ray fluoroscopy guidance. However, current techniques for ablating complex arrhythmias such as atrial fibrillation and ventricular tachycardia are associated with sub-optimal success rates and prolonged radiation exposure. Pre-procedure 3-D magnetic resonance imaging (MRI) has improved understanding of the anatomic basis of complex arrhythmias and is being used for planning and guidance of ablation procedures. A particular strength of MRI compared to other imaging modalities is the ability to visualize ablation lesions. Post-procedure MRI is now being applied to assess ablation lesion location and permanence with the goal of identifying factors leading to procedure success and failure. In the future, intra-procedure real-time MRI, together with the ability to image complex 3-D arrhythmogenic anatomy and target additional ablation to regions of incomplete lesion formation, may allow for more successful treatment of even complex arrhythmias without exposure to ionizing radiation. Development of clinical grade MRI-compatible electrophysiology devices is required to transition intra-procedure MRI from preclinical studies to more routine use in patients.
Keywords: ablation; arrhythmia; electrophysiology; magnetic resonance imaging.
Figures
References
-
- Calkins H, Yong P, Miller JM, et al. Catheter ablation of accessory pathways, atrioventricular nodal reentrant tachycardia, and the atrioventricular junction: final results of a prospective, multicenter clinical trial. The Atakr Multicenter Investigators Group. Circulation. 1999;99:262–70. - PubMed
-
- Shah DC, Jais P, Haissaguerre M, et al. Three-dimensional mapping of the common atrial flutter circuit in the right atrium. Circulation. 1997;96:3904–12. - PubMed
-
- Pappone C, Rosanio S, Oreto G, et al. Circumferential radiofrequency ablation of pulmonary vein ostia: A new anatomic approach for curing atrial fibrillation. Circulation. 2000;102:2619–28. - PubMed
-
- Marchlinski FE, Callans DJ, Gottlieb CD, Zado E. Linear ablation lesions for control of unmappable ventricular tachycardia in patients with ischemic and nonischemic cardiomyopathy. Circulation. 2000;101:1288–96. - PubMed
LinkOut - more resources
Full Text Sources