

Milestones in the evolution of hepatic surgery
- PMID: 23908793
- PMCID: PMC3678786
- DOI: 10.5041/RMMJ.10021
Milestones in the evolution of hepatic surgery
Abstract
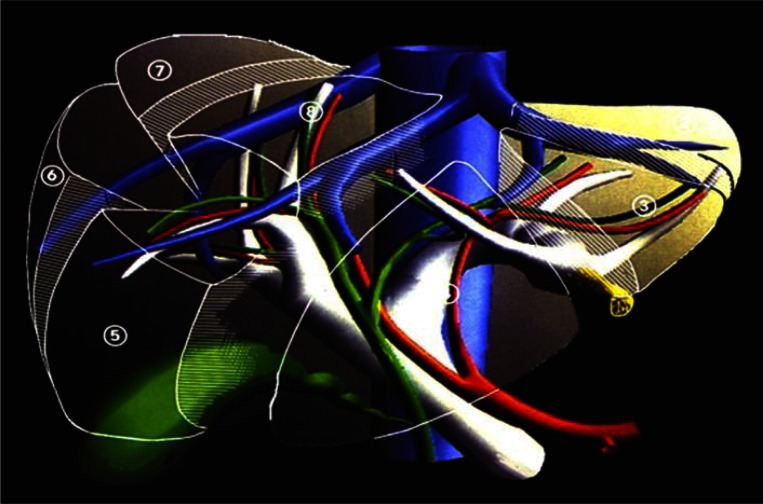
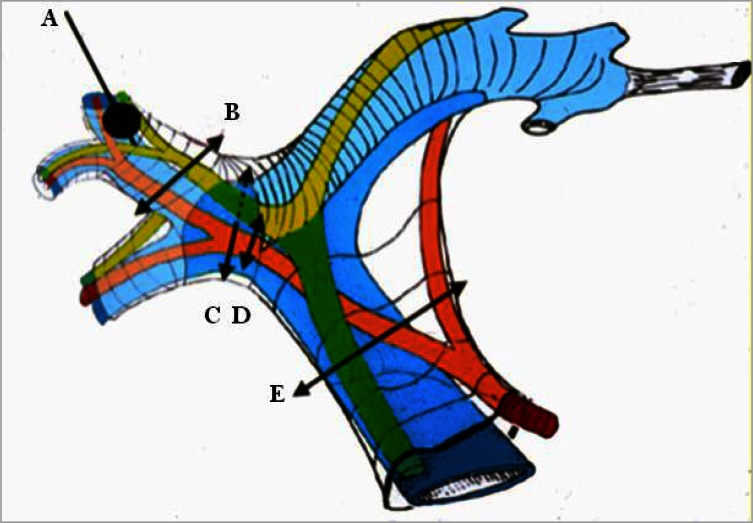
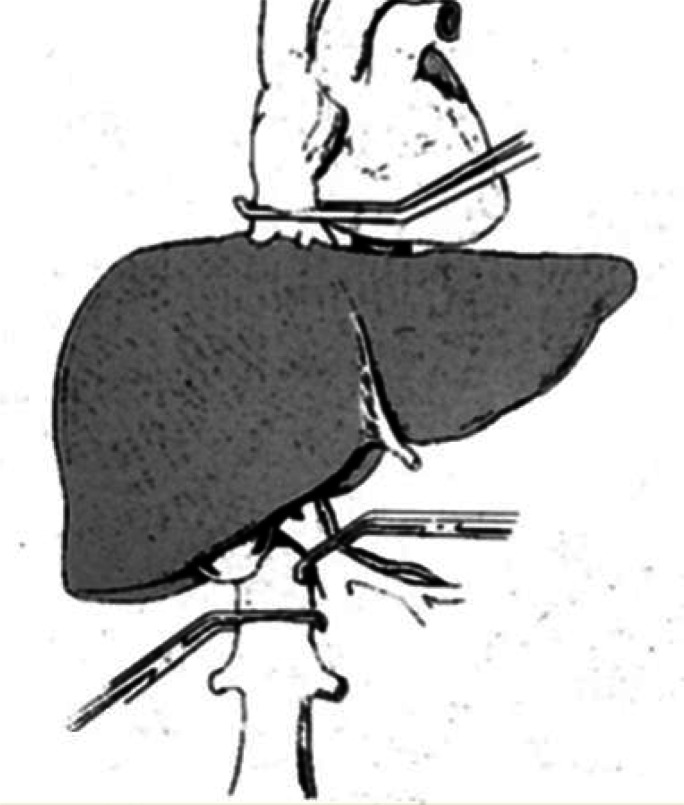
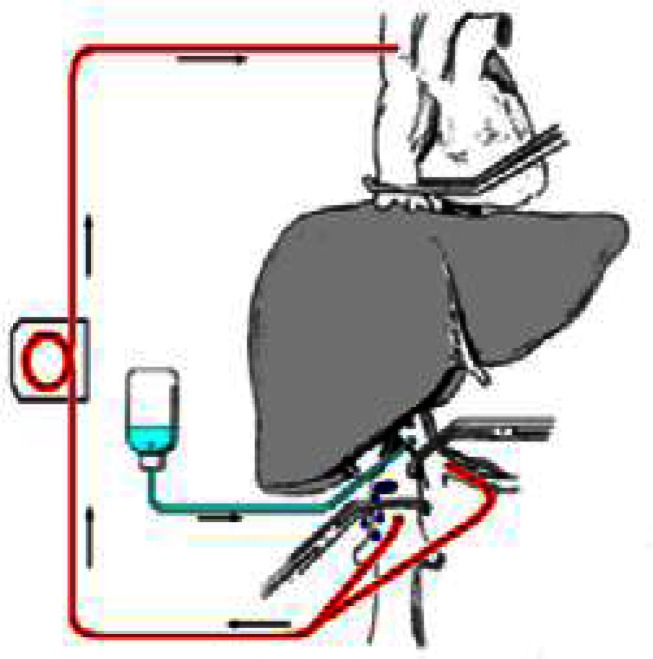
This paper describes the rapid evolution of modern liver surgery, starting in the middle of the twentieth century. Claude Couinaud studied and described the segmental anatomy of the liver, Thomas Starzl performed the first liver transplantations, and Henri Bismuth introduced the concept of anatomical resections. Hepatic surgery has developed significantly since those early days. To date, innovative techniques are applied, using cutting-edge technologies: Intraoperative ultrasound, techniques of vascular exclusion of the liver, new devices for performing homeostasis and dissection, laparoscopy for resections, and new drugs that allow the resection of previously unresectable tumors. The next stage in liver surgery will probably be the implementation of a multidisciplinary holistic approach to the liver-diseased patient that will ensure the best and most efficient treatments in the future.
Keywords: Surgery; liver; transection; transplantation.
Figures
References
-
- Langenbuch C. Ein Fall von Resecktion eines linksseitigen Schnurlappens der Leber. Berl Klin Wochenschr. 1888;25:37. German.
-
- Lortat-Jacob JL, Robert HG. Well defined technic for right hepatectomy. Presse Med. 1952;60:549–51. French. - PubMed
-
- Couinaud C. Lobes et segments hépatiques. Presse Med. 1954;62:709. French. - PubMed
LinkOut - more resources
Full Text Sources