

Coarctation of the aorta - the current state of surgical and transcatheter therapies
- PMID: 23909637
- PMCID: PMC3780346
- DOI: 10.2174/1573403x113099990032
Coarctation of the aorta - the current state of surgical and transcatheter therapies
Abstract
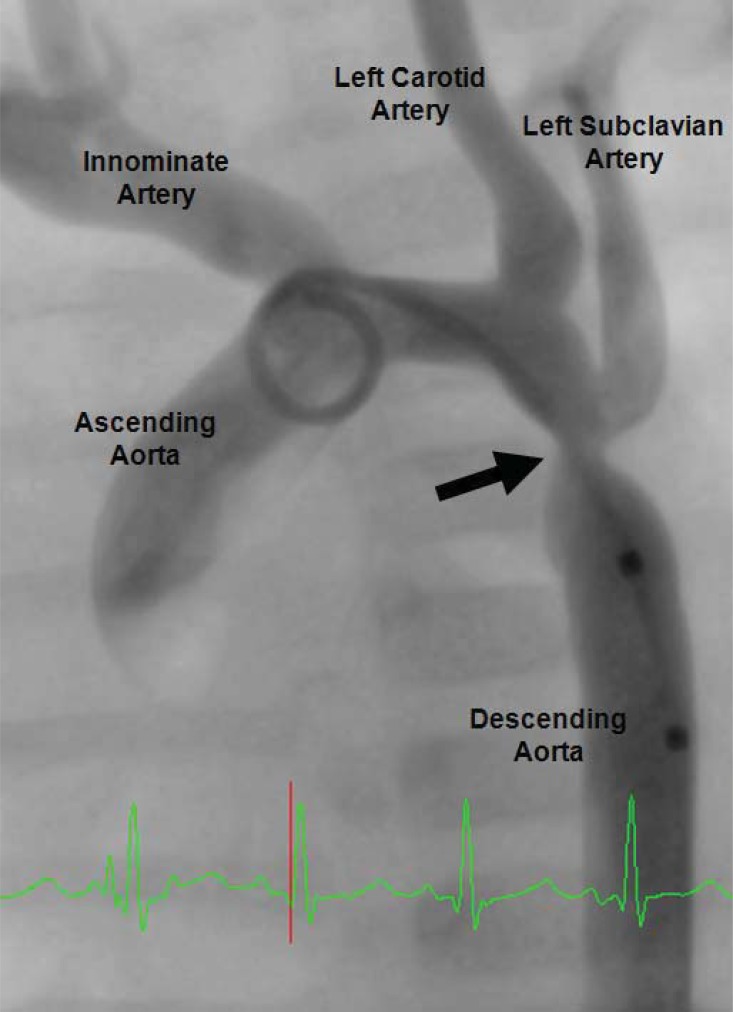
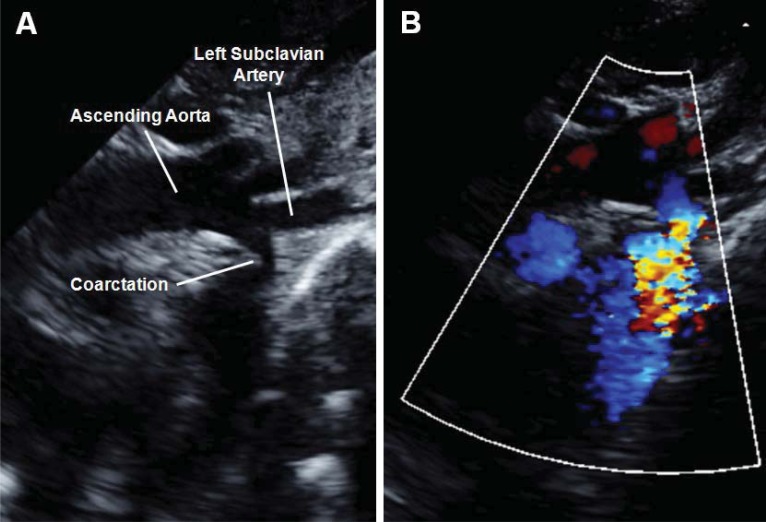
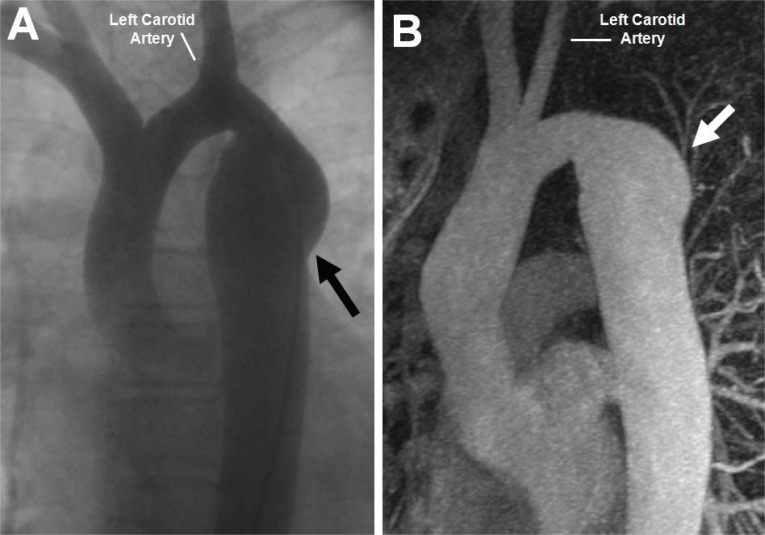
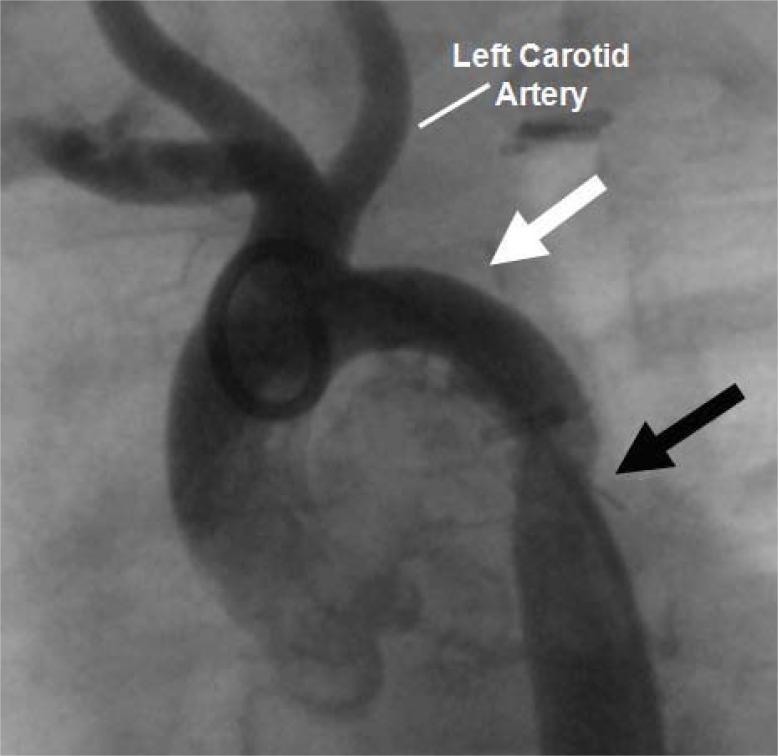
Aortic coarctation represents a distinct anatomic obstruction as blood moves from the ascending to the descending aorta and can present in a range of ages from infancy to adulthood. While it is often an isolated and discrete narrowing, it can also be seen in the more extreme scenario of severe arch hypoplasia as seen in the hypoplastic left heart syndrome or in conjunction with numerous other congenital heart defects. Since the first description of an anatomic surgical repair over sixty years ago, an evolution of both surgical and transcatheter therapies has occurred allowing clinicians to manage and treat this disease with excellent results and low morbidity and mortality. This review focuses on the current state of both transcatheter and surgical therapies, paying special attention to recent data on long-term follow-up of both approaches. Further, current thoughts will be explored about future therapeutic options that attempt to improve upon historical long-term outcomes.
Figures


References
-
- Kieth J, Rowe R, Vlad P. Heart Disease in Infancy and Childhood. 1958;1:877.
-
- Folger GM, Stein PD. Bicuspid aortic valve morphology when associated with coarctation of the aorta. Catheter Cardiovasc Diag. 1984;10(1):17–25. - PubMed
-
- Shone JD, Sellers RD, Anderson RC, Adams P, Lillehei CW, Edwards J. The developmental complex of “parachute mitral valve,” supravalvular ring of left atrium, subaortic stenosis, and coarctation of aorta. Am J Cardiol. 1963;11:714–25. - PubMed
-
- Machii M, Becker A. Nature of coarctation in hypoplastic left heart syndrome. Ann Thorac Surg. 1995;59(6):1491–4. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
