

Adult obstructive sleep apnoea
- PMID: 23910433
- PMCID: PMC3909558
- DOI: 10.1016/S0140-6736(13)60734-5
Adult obstructive sleep apnoea
Abstract
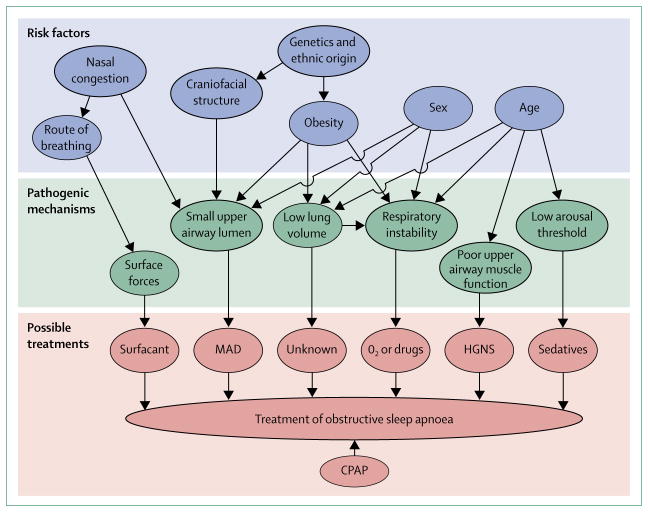
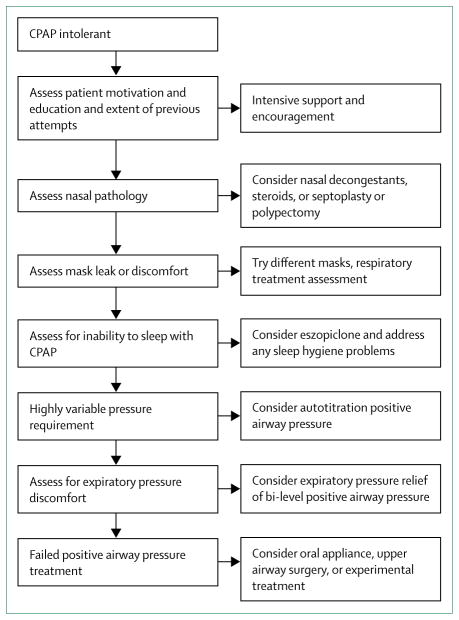
Obstructive sleep apnoea is an increasingly common disorder of repeated upper airway collapse during sleep, leading to oxygen desaturation and disrupted sleep. Features include snoring, witnessed apnoeas, and sleepiness. Pathogenesis varies; predisposing factors include small upper airway lumen, unstable respiratory control, low arousal threshold, small lung volume, and dysfunctional upper airway dilator muscles. Risk factors include obesity, male sex, age, menopause, fluid retention, adenotonsillar hypertrophy, and smoking. Obstructive sleep apnoea causes sleepiness, road traffic accidents, and probably systemic hypertension. It has also been linked to myocardial infarction, congestive heart failure, stroke, and diabetes mellitus though not definitively. Continuous positive airway pressure is the treatment of choice, with adherence of 60-70%. Bi-level positive airway pressure or adaptive servo-ventilation can be used for patients who are intolerant to continuous positive airway pressure. Other treatments include dental devices, surgery, and weight loss.
Copyright © 2014 Elsevier Ltd. All rights reserved.
Conflict of interest statement
AM has received consulting and research income from Philips, Sleep Group Solutions, Pfizer, Apnex Medical, and Apnicure but has relinquished all outside personal income since May 2012. DGM has received funding from the American Heart Association. ASJ is funded by the Australian Research Council and NHMRC Australia. Before 2010, she received consulting income from Apnex Medical.
Figures
References
-
- Malhotra A, White DP. Obstructive sleep apnoea. Lancet. 2002;360:237–45. - PubMed
-
- Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. The occurrence of sleep-disordered breathing among middle-aged adults. N Engl J Med. 1993;32:1230–35. - PubMed
-
- Sforza E, Chouchou F, Collet P, Pichot V, Barthelemy JC, Roche F. Sex differences in obstructive sleep apnoea in an elderly French population. Eur Respir J. 2011;37:1137–43. - PubMed
-
- Young T, Peppard P, Gottlieb D. The epidemiology of obstructive sleep apnea: a population health perspective. Am J Respir Crit Care Med. 2002;165:1217–39. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
