

Orthogeriatric care models and outcomes in hip fracture patients: a systematic review and meta-analysis
- PMID: 23912859
- PMCID: PMC3909556
- DOI: 10.1097/BOT.0b013e3182a5a045
Orthogeriatric care models and outcomes in hip fracture patients: a systematic review and meta-analysis
Abstract
Objectives: Hip fractures are common, morbid, and costly health events that threaten independence and function of older patients. The purpose of this systematic review and meta-analysis was to determine if orthogeriatric collaboration models improve outcomes.
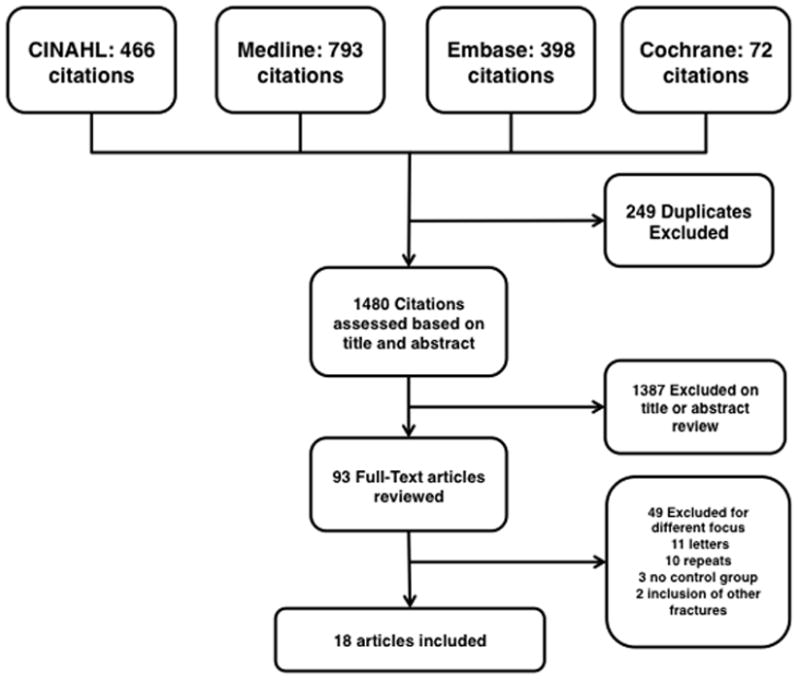
Data sources: Articles in English and Spanish languages were searched in the electronic databases including MEDLINE, Cumulative Index to Nursing and Allied Health Literature (CINAHL), EMBASE, and the Cochrane Registry from 1992 to 2012.
Study selection: Studies were included if they described an inpatient multidisciplinary approach to hip fracture management involving an orthopaedic surgeon and a geriatrician. Studies were grouped into 3 following categories: routine geriatric consultation, geriatric ward with orthopaedic consultation, and shared care. After independent review of 1480 citations by 2 authors, 18 studies (9094 patients) were identified as meeting the inclusion criteria.
Data extraction: In-hospital mortality, length of stay, and long-term mortality outcomes were collected.
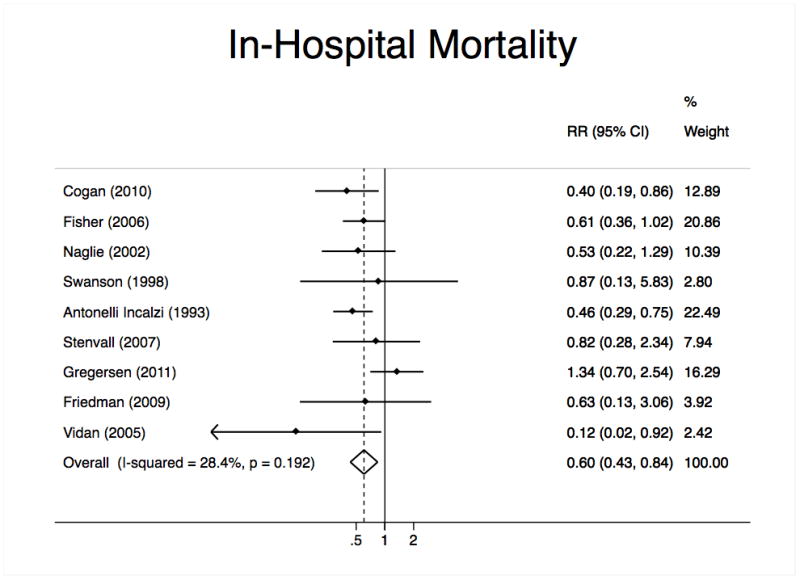
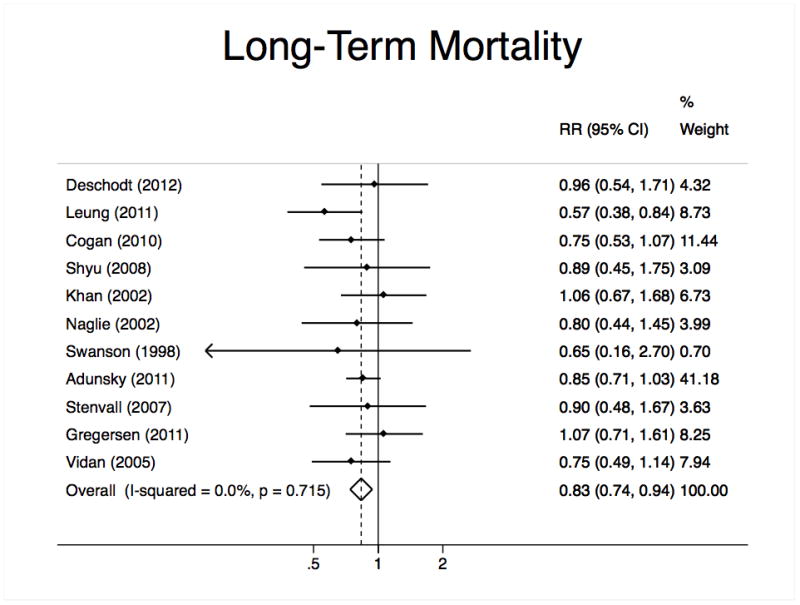
Data synthesis: A random effects model meta-analysis determined whether orthogeriatric collaboration was associated with improved outcomes. The overall meta-analysis found that orthogeriatric collaboration was associated with a significant reduction of in-hospital mortality [relative risk 0.60; 95% confidence interval (95% CI), 0.43-0.84) and long-term mortality (relative risk 0.83; 95% CI, 0.74-0.94). Length of stay (standardized mean difference -0.25; 95% CI, -0.44 to -0.05) was significantly reduced, particularly in the shared care model (standardized mean difference -0.61; 95% CI, -0.95 to -0.28), but heterogeneity limited this interpretation. Other variables such as time to surgery, delirium, and functional status were measured infrequently.
Conclusions: This meta-analysis supports orthogeriatric collaboration to improve mortality after hip repair. Further study is needed to determine the best model of orthogeriatric collaboration and if these partnerships improve functional outcomes.
Conflict of interest statement
Dr. Javedan works for an ortho-geriatric co-management service at Brigham and Women’s Hospital. The authors have no other financial conflicts of interest to declare.
Support for this research was made possible through NIH grant #: 1T35AG038027-02. Dr. Rudolph is supported by a VA Rehabilitation Research and Development Career Development Award.
Presented in part at the American Geriatric Society Meeting, Grapevine, TX, May 3, 2013.
Figures
References
-
- Gullberg B, Johnell O, Kanis JA. World-wide projections for hip fracture. Osteoporosis International. 1997;7:407–13. - PubMed
-
- Butler M, Forte M, Kane RL, et al. AHRQ Publication No 09–E013. Rockville, MD: Agency for Healthcare Research and Quality; Aug, 2009. Treatment of common hip fractures. Evidence Report/Technology Assessment, No. 184. - PubMed
-
- Zuckerman JD. Hip fracture. N Engl J Med. 1996;334:1519–25. - PubMed
-
- Leibson CL, Tosteson AN, Gabriel SE, Ransom JE, Melton LJ. Mortality, disability, and nursing home use for persons with and without hip fracture: a population-based study. J Am Geriatr Soc. 2002;50:1644–50. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
