

Defining a threshold for intervention in breast cancer-related lymphedema: what level of arm volume increase predicts progression?
- PMID: 23912961
- PMCID: PMC3788652
- DOI: 10.1007/s10549-013-2655-2
Defining a threshold for intervention in breast cancer-related lymphedema: what level of arm volume increase predicts progression?
Abstract
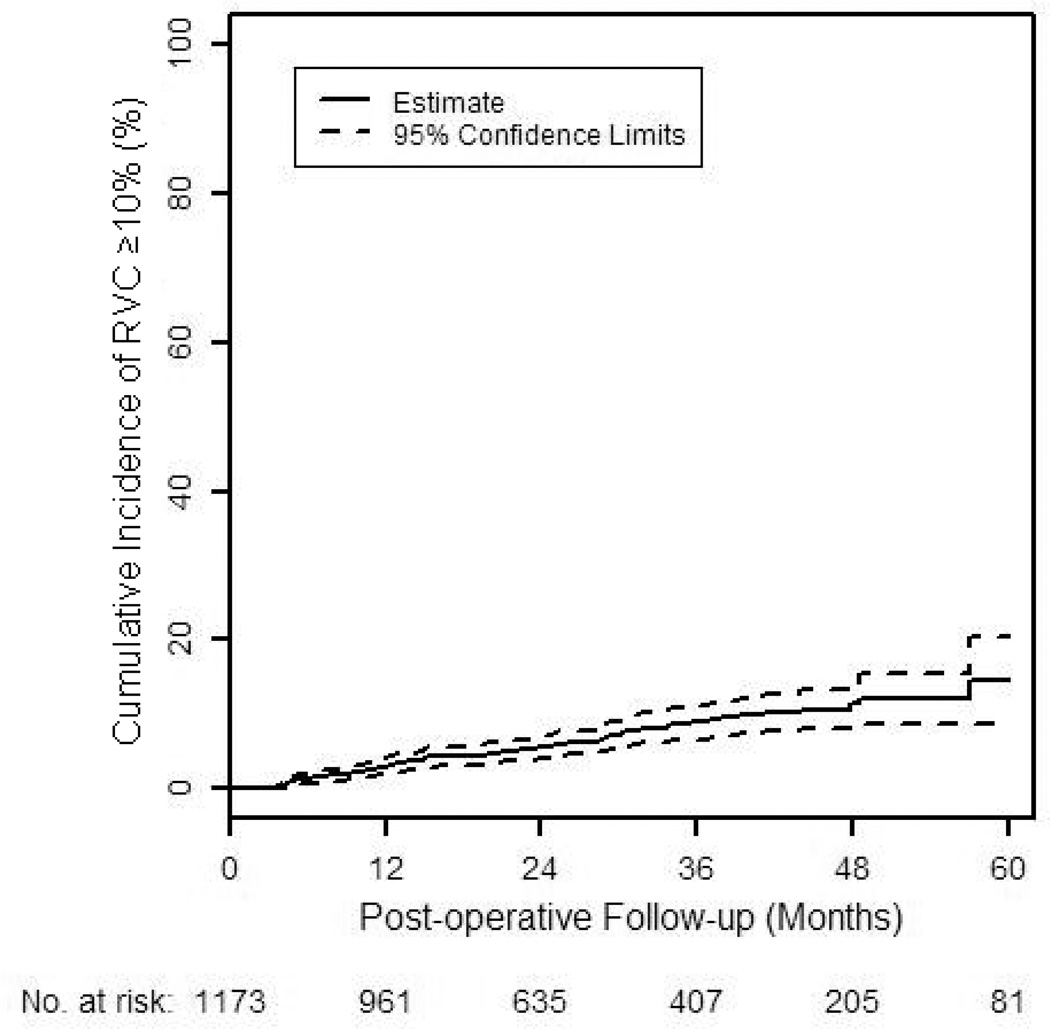
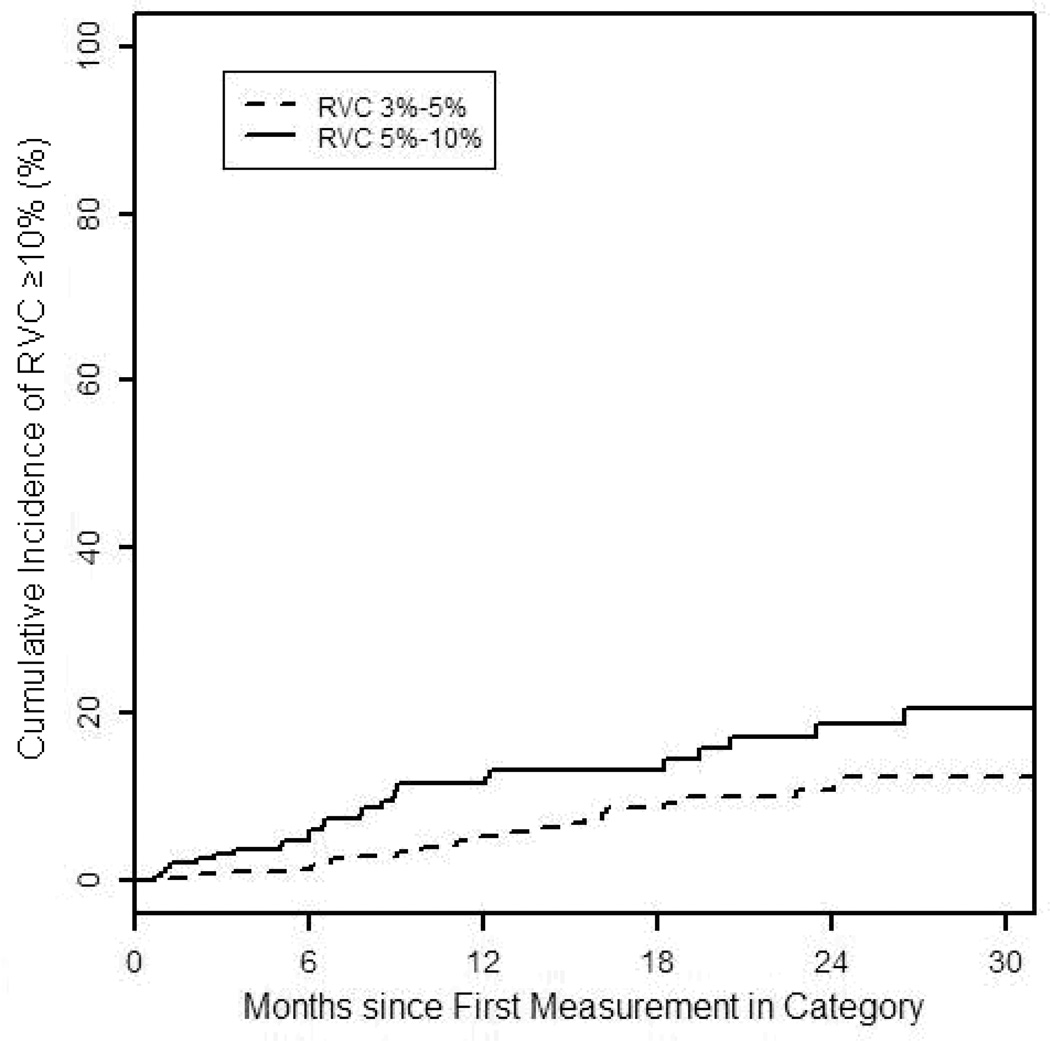
The purpose of this study is to evaluate arm volume measurements and clinico-pathologic characteristics of breast cancer patients to define a threshold for intervention in breast cancer-related lymphedema. We prospectively performed arm volume measurements on breast cancer patients using a Perometer. Arm measurements were performed pre- and post-operatively, and change in arm volume was quantified using a relative volume change (RVC) equation. Patient and treatment risk factors were evaluated. Cox proportional hazards models with time-dependent covariates for RVC were used to evaluate whether RVC elevations of ≥3 to <5 % or ≥5 to <10 % occurring ≤3 months or >3 months after surgery were associated with progression to ≥10 % RVC. 1,173 patients met eligibility criteria with a median of 27 months post-operative follow-up. The cumulative incidence of ≥10 % RVC at 24 months was 5.26 % (95 % CI 4.01-6.88 %). By multivariable analysis, a measurement of ≥5 to <10 % RVC occurring >3 months after surgery was significantly associated with an increased risk of progression to ≥10 % RVC (HR 2.97, p < 0.0001), but a measurement of ≥3 to <5 % RVC during the same time period was not statistically significantly associated (HR 1.55, p = 0.10). Other significant risk factors included a measurement ≤3 months after surgery with RVC of ≥3 to <5 % (p = 0.007), ≥5 to <10 % (p < 0.0001), or ≥10 % (p = 0.023), axillary lymph node dissection (ALND) (p < 0.0001), and higher BMI at diagnosis (p = 0.0028). Type of breast surgery, age, number of positive or number of lymph nodes removed, nodal radiation, chemotherapy, and hormonal therapy were not significant (p > 0.05). Breast cancer patients who experience a relative arm volume increase of ≥3 to <5 % occurring >3 months after surgery do not have a statistically significant increase in risk of progression to ≥10 %, a common lymphedema criterion. Our data support utilization of a ≥5 to <10 % threshold for close monitoring or intervention, warranting further assessment. Additional risk factors for progression to ≥10 % include ALND, higher BMI, and post-operative arm volume elevation.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Khan F, Amatya B, Pallant JF, Rajapaksa I. Factors associated with long-term functional outcomes and psychological sequelae in women after breast cancer. Breast. 2012;(3):314–320. - PubMed
-
- Sakorafas GH, Peros G, Cataliotti L, Vlastos G. Lymphedema following axillary lymph node dissection for breast cancer. Surg Oncol. 2006;15(3):153–165. - PubMed
-
- Hayes SC, Janda M, Cornish B, Battistutta D, Newman B. Lymphedema after breast cancer: incidence, risk factors, and effect on upper body function. J Clin Oncol. 2008;26(21):3536–3542. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
