

Surgical treatment for total root avulsion type brachial plexus injuries by neurotization: a prospective comparison study between total and hemicontralateral C7 nerve root transfer
- PMID: 23913440
- PMCID: PMC4282479
- DOI: 10.1002/micr.22148
Surgical treatment for total root avulsion type brachial plexus injuries by neurotization: a prospective comparison study between total and hemicontralateral C7 nerve root transfer
Abstract
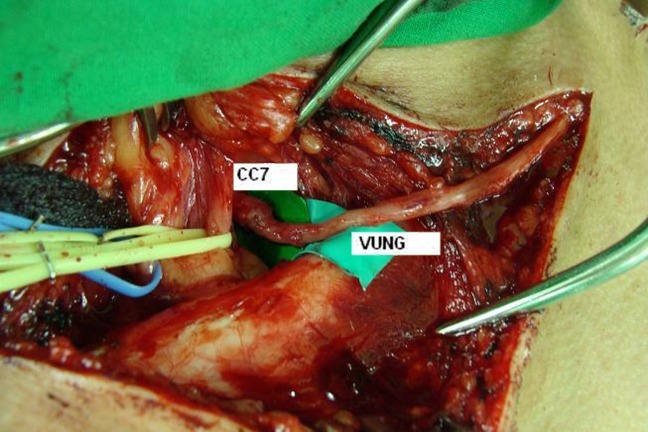
Purpose: We conducted a clinical study to evaluate the effects of neurotization, especially comparing the total contralateral C7 (CC7) root transfer to hemi-CC7 transfer, on total root avulsion brachial plexus injuries (BPI).
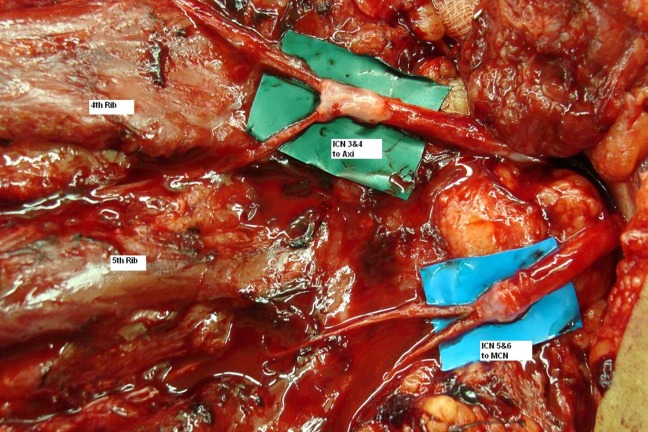
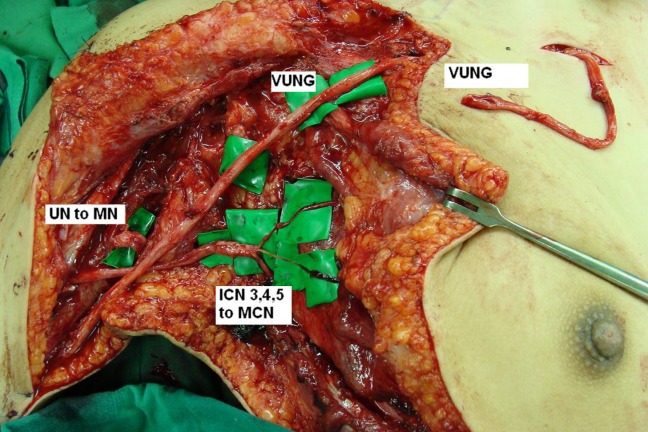
Methods: Forty patients who received neurotization for BPI were enrolled in this prospective study. Group 1 (n = 20) received hemi-CC7 transfer for hand function, while group 2 (n = 20) received total-CC7 transfer. Additional neurotization included spinal accessory, phrenic, and intercostal nerve transfer for shoulder and elbow function. The results were evaluated with an average of 6 years follow-up.
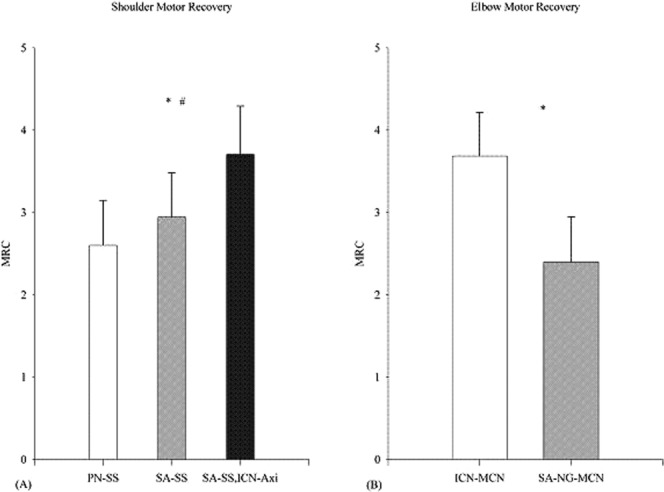
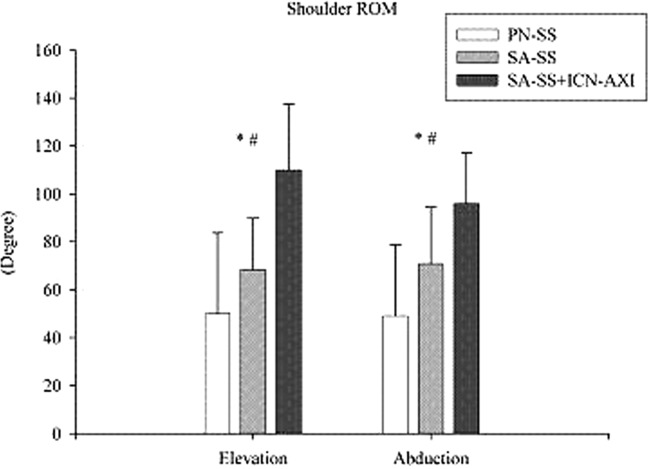
Results: Group 1 had fewer donor site complications (15%) than group 2 (45%); group 2 had significantly better hand M3 and M4 motor function (65%) than group 1 (30%; P = 0.02). There was no difference in sensory recovery. Significantly, better shoulder function was obtained by simultaneous neurotization on both suprascapular and axillary nerves.
Conclusions: Total-CC7 transfer had better hand recovery but more donor complications than hemi-CC7. Neurotization on both supra-scapular and axillary nerves improved shoulder recovery.
Copyright © 2013 Wiley Periodicals, Inc.
Figures




References
-
- Gu YD, Zhang GM, Chen DS, Yan JG, Cheng XM, Chen L. Seventh cervical nerve root transfer from the contralateral healthy side for treatment of brachial plexus root avulsion. J Hand Surg Br. 1992;17:518–521. - PubMed
-
- Tu YK, Chung KC. Surgical procedures for recovery of hand function. In: Chung KC, Yang LJS, McGillicuddy JE, editors. Practical management of pediatric and adult brachial plexus palsies. Saunders Elsevier, New York; 2012. pp. 271–300.
-
- Songcharoen P, Wongtrakul S, Mahaisavariya B, Spinner RJ. Hemi-contralateral C7 transfer to median nerve in the treatment of root avulsion brachial plexus injury. J Hand Surg Am. 2001;26:1058–1064. - PubMed
-
- Thomeer RT, Malessy MJ. Surgical repair of brachial plexus injury. Clin Neurol Neurosurg. 1993;95(Suppl):S65–S72. - PubMed
-
- Bonnard C, Anastakis DI. Complete palsy. In: Alain Gilbert., editor. Brachial plexus injuries. London: Martin Dunitz; 2001. pp. 67–75.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
