

Chronic baroreflex activation restores spontaneous baroreflex control and variability of heart rate in obesity-induced hypertension
- PMID: 23913707
- PMCID: PMC3798752
- DOI: 10.1152/ajpheart.00464.2013
Chronic baroreflex activation restores spontaneous baroreflex control and variability of heart rate in obesity-induced hypertension
Abstract
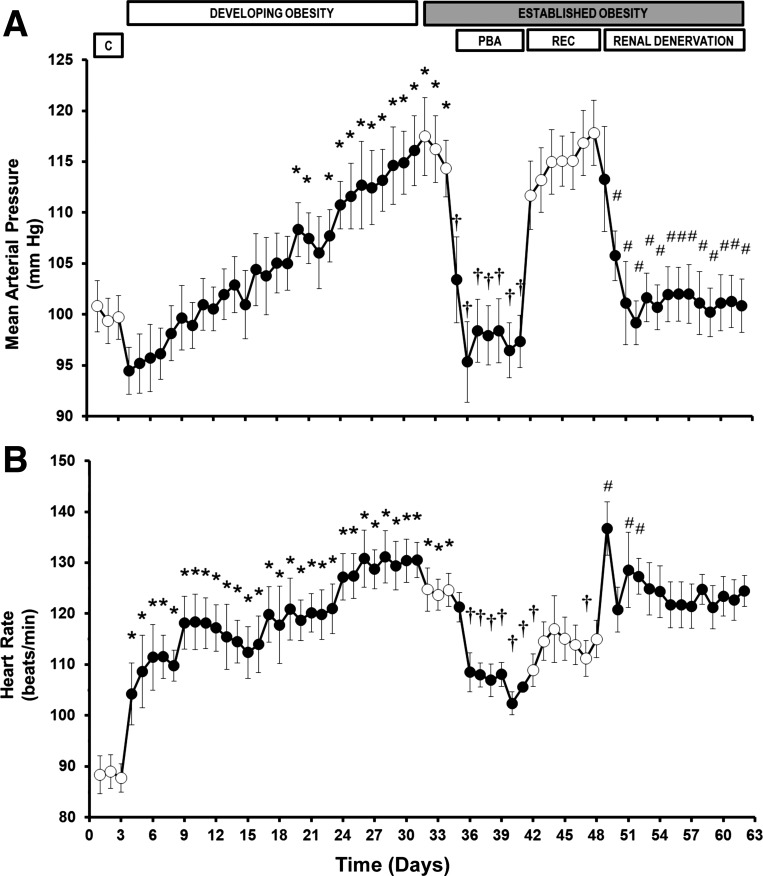
The sensitivity of baroreflex control of heart rate is depressed in subjects with obesity hypertension, which increases the risk for cardiac arrhythmias. The mechanisms are not fully known, and there are no therapies to improve this dysfunction. To determine the cardiovascular dynamic effects of progressive increases in body weight leading to obesity and hypertension in dogs fed a high-fat diet, 24-h continuous recordings of spontaneous fluctuations in blood pressure and heart rate were analyzed in the time and frequency domains. Furthermore, we investigated whether autonomic mechanisms stimulated by chronic baroreflex activation and renal denervation-current therapies in patients with resistant hypertension, who are commonly obese-restore cardiovascular dynamic control. Increases in body weight to ∼150% of control led to a gradual increase in mean arterial pressure to 17 ± 3 mmHg above control (100 ± 2 mmHg) after 4 wk on the high-fat diet. In contrast to the gradual increase in arterial pressure, tachycardia, attenuated chronotropic baroreflex responses, and reduced heart rate variability were manifest within 1-4 days on high-fat intake, reaching 130 ± 4 beats per minute (bpm) (control = 86 ± 3 bpm) and ∼45% and <20%, respectively, of control levels. Subsequently, both baroreflex activation and renal denervation abolished the hypertension. However, only baroreflex activation effectively attenuated the tachycardia and restored cardiac baroreflex sensitivity and heart rate variability. These findings suggest that baroreflex activation therapy may reduce the risk factors for cardiac arrhythmias as well as lower arterial pressure.
Keywords: baroreflex; heart rate variability; hypertension; obesity; sympathetic nervous system.
Figures




References
-
- Alvarez GE, Davy BM, Ballard TP, Beske SD, Davy KP. Weight loss increases cardiovagal baroreflex function in obese and older men. Am J Physiol Endocrinol Metab 289: E665–E669, 2005 - PubMed
-
- Aronne LJ, Mackintosh R, Rosenbaum M, Leibel RL, Hirsch J. Autonomic nervous system activity in weight gain and weight loss. Am J Physiol Regul Integr Comp Physiol 269: R222–R225, 1995 - PubMed
-
- Benjamin EJ, Wolf PA, D'Agostino RB, Silbershatz H, Kannel WB, Levy D. Impact of atrial fibrillation on the risk of death: the Framingham Heart Study. Circulation 98: 946–952, 1998 - PubMed
-
- Bernston GG, Bigger JT, Jr, Eckberg DL, Grossman P, Kaufmann PG, Malik M, Nagaraja HN, Porges SW, Saul JP, Stone PH, van der Molen MW. Heart rate variability: origins, methods, and interpretive caveats. Psychophysiology 34: 623–648, 1997 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical