

Pitfalls associated with the diagnosis of herpes simplex encephalitis
- PMID: 23914095
- PMCID: PMC3724297
- DOI: 10.4103/0976-3147.112756
Pitfalls associated with the diagnosis of herpes simplex encephalitis
Abstract
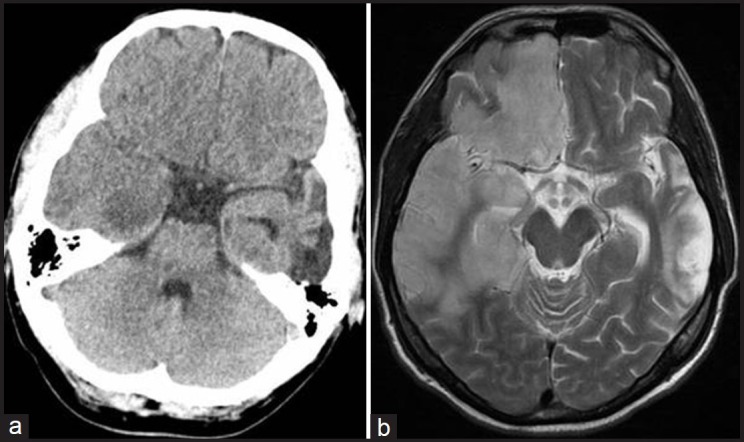
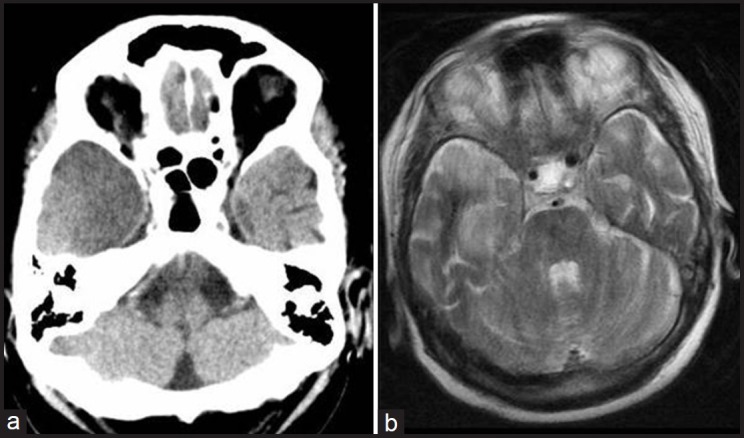
Herpes simplex encephalitis (HSE) still remains a serious illness with high morbidity and mortality. The characteristic presentation of HSE usually consists of fever, headache, and altered mental function. We present three patients with atypical features of HSE. First, a 48-year-old man with symptomatic posttraumatic epilepsy, who developed a gastrointestinal infection, seizures, and fever. After significant clinical improvement, the patient had fever again and developed a status epilepticus, which led to the diagnosis of HSE. Second, an 84-year-old woman with hyperactive delirium after levofloxacin intake. Cranial computed tomography (CCT) revealed hypodense temporal changes, prompting lumbar puncture and diagnosis of HSE. Third, a 51-year-old diabetic woman presented with fever and acute confusion. As CCT and cell count of cerebrospinal fluid (CSF) were normal, infection and hyperglycemia as initial diagnoses were postulated. Due to aphasic symptoms, the differential diagnosis of a stroke was taken into account. Thus a second lumbar puncture led to the correct diagnosis of HSE. These atypical presentations need a high grade of suspicion and a high willingness to reconsider the initial working diagnosis, in order to prevent a diagnostic delay.
Keywords: Acyclovir; atypical course of disease; cerebrospinal fluid; consciousness disturbance; herpes simplex encephalitis; herpes simplex virus.
Conflict of interest statement
Figures

References
-
- Steiner I, Budka H, Chaudhuri A, Koskiniemi M, Sainio K, Salonen O, et al. Viral encephalitis: A review of diagnostic methods and guidelines for management. Eur J Neurol. 2005;12:331–43. - PubMed
-
- Whitley RJ. Herpes simplex encephalitis: Adolescents and adults. Antiviral Res. 2006;71:141–8. - PubMed
-
- Stahl JP, Mailles A, De Broucker T. Herpes simplex encephalitis and management of acyclovir in encephalitis patients in France. Epidemiol Infect. 2012;140:372–81. - PubMed
-
- Fodor PA, Levin MJ, Weinberg A, Sandberg E, Sylman J, Tyler KL. Atypical herpes simplex virus encephalitis diagnosed by PCR amplification of viral DNA from CSF. Neurology. 1998;51:554–9. - PubMed
-
- Tunkel AR, Glaser CA, Bloch KC, Sejvar JJ, Marra CM, Roos KL, et al. The management of encephalitis: Clinical practice guidelines by the Infectious Diseases Society of America. Clin Infect Dis. 2008;47:303–27. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials