

Therapeutic interventions for increasing ankle dorsiflexion after ankle sprain: a systematic review
- PMID: 23914912
- PMCID: PMC3784372
- DOI: 10.4085/1062-6050-48.4.11
Therapeutic interventions for increasing ankle dorsiflexion after ankle sprain: a systematic review
Abstract
Context: Clinicians perform therapeutic interventions, such as stretching, manual therapy, electrotherapy, ultrasound, and exercises, to increase ankle dorsiflexion. However, authors of previous studies have not determined which intervention or combination of interventions is most effective.
Objective: To determine the magnitude of therapeutic intervention effects on and the most effective therapeutic interventions for restoring normal ankle dorsiflexion after ankle sprain.
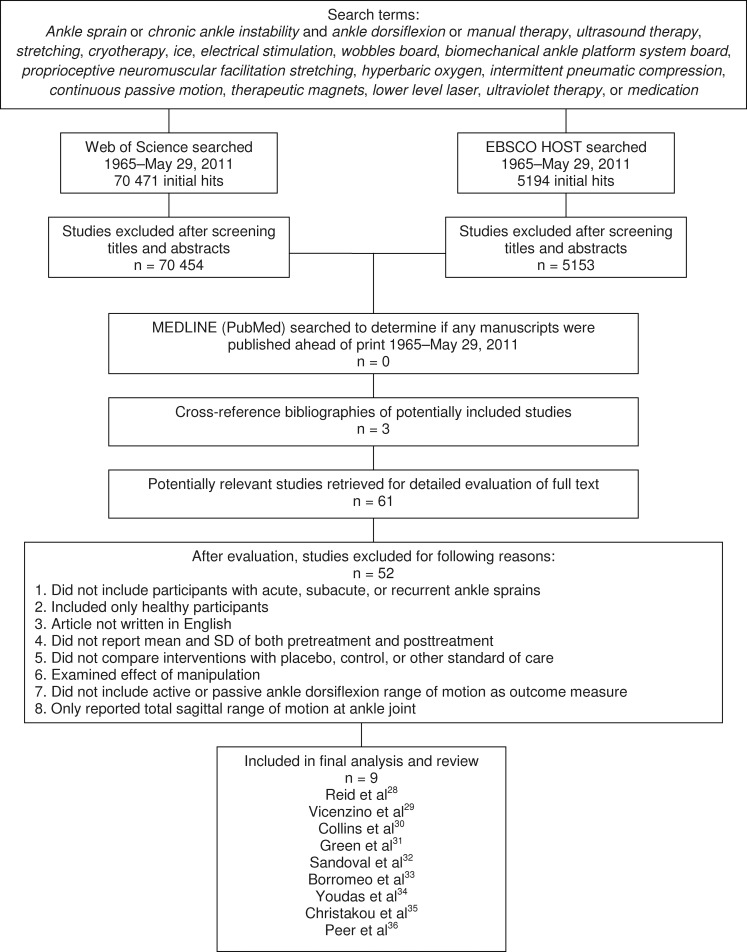
Data sources: We performed a comprehensive literature search in Web of Science and EBSCO HOST from 1965 to May 29, 2011, with 19 search terms related to ankle sprain, dorsiflexion, and intervention and by cross-referencing pertinent articles.
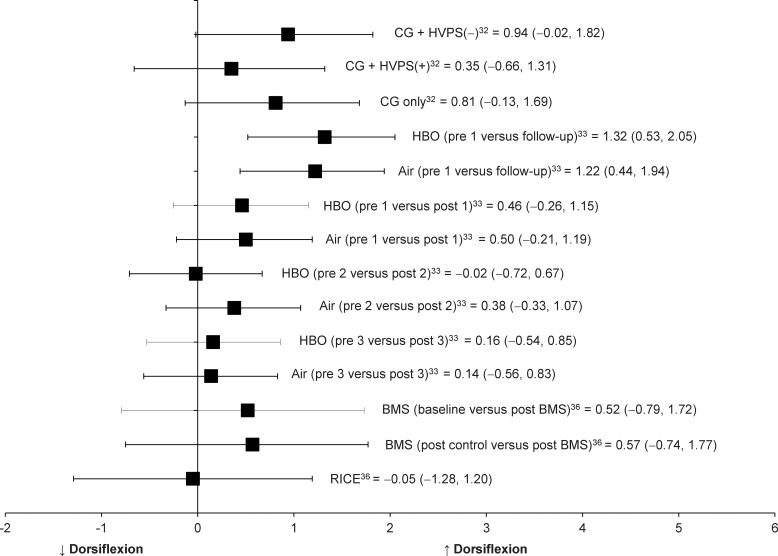
Study selection: Eligible studies had to be written in English and include the means and standard deviations of both pretreatment and posttreatment in patients with acute, subacute, or chronic ankle sprains. Outcomes of interest included various joint mobilizations, stretching, local vibration, hyperbaric oxygen therapy, electrical stimulation, and mental-relaxation interventions.
Data extraction: We extracted data on dorsiflexion improvements among various therapeutic applications by calculating Cohen d effect sizes with associated 95% confidence intervals (CIs) and evaluated the methodologic quality using the Physiotherapy Evidence Database (PEDro) scale.
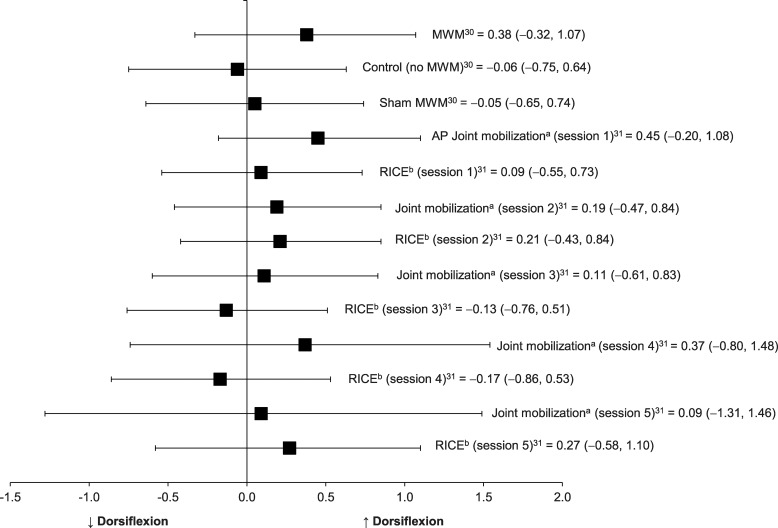
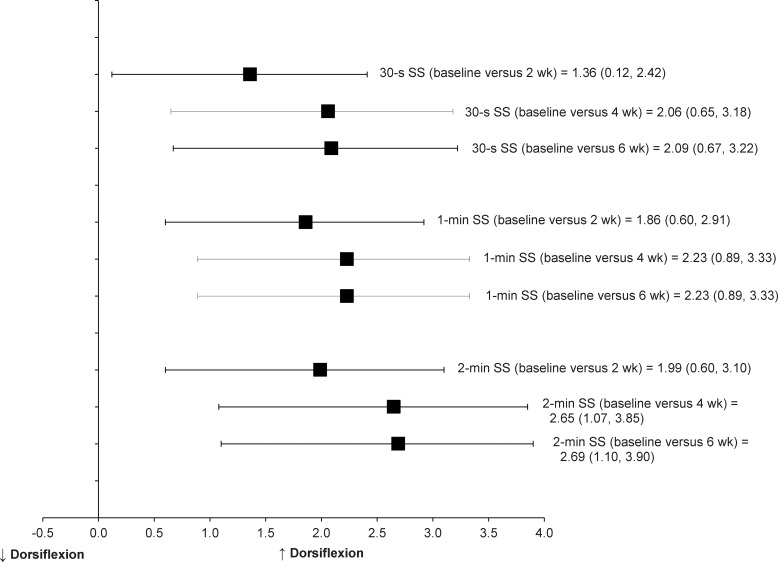
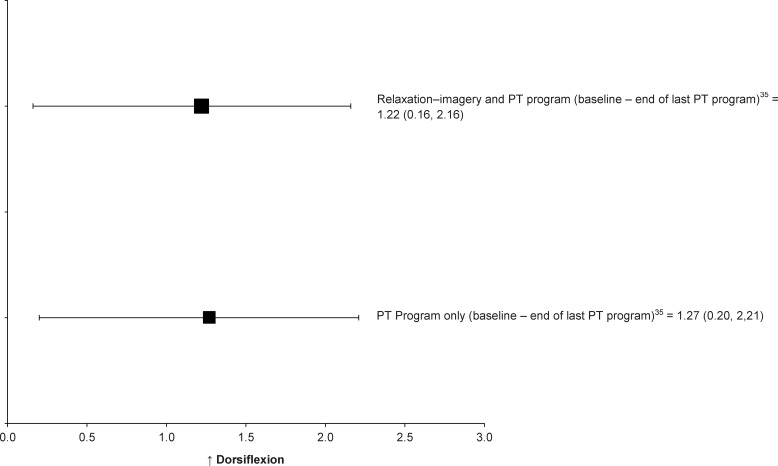
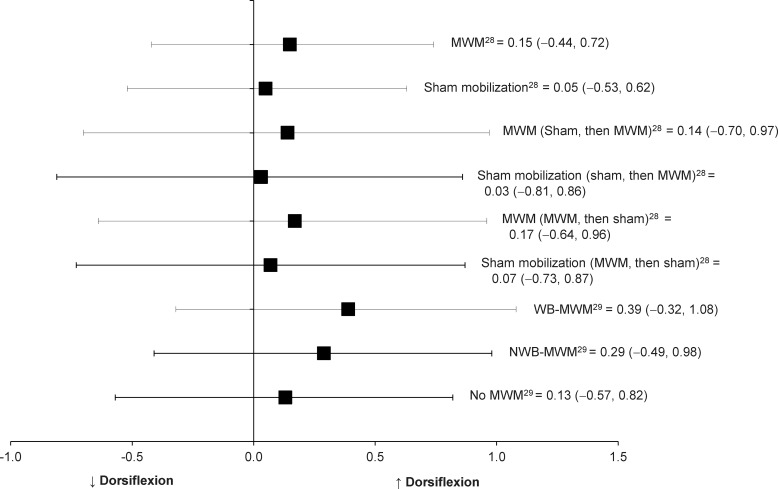
Data synthesis: In total, 9 studies (PEDro score = 5.22 ± 1.92) met the inclusion criteria. Static-stretching interventions with a home exercise program had the strongest effects on increasing dorsiflexion in patients 2 weeks after acute ankle sprains (Cohen d = 1.06; 95% CI = 0.12, 2.42). The range of effect sizes for movement with mobilization on ankle dorsiflexion among individuals with recurrent ankle sprains was small (Cohen d range = 0.14 to 0.39).
Conclusions: Static-stretching intervention as a part of standardized care yielded the strongest effects on dorsiflexion after acute ankle sprains. The existing evidence suggests that clinicians need to consider what may be the limiting factor of ankle dorsiflexion to select the most appropriate treatments and interventions. Investigators should examine the relationship between improvements in dorsiflexion and patient progress using measures of patient self-reported functional outcome after therapeutic interventions to determine the most appropriate forms of therapeutic interventions to address ankle-dorsiflexion limitation.
Figures
References
-
- Fernandez WG, Yard EE, Comstock RD. Epidemiology of lower extremity injuries among U.S. high school athletes. Acad Emerg Med. 2007;14(7):641–645. - PubMed
-
- Fong DT, Hong Y, Chan LK, Yung PS, Chan KM. A systematic review on ankle injury and ankle sprain in sports. Sports Med. 2007;37(1):73–94. - PubMed
-
- Baumhauer JF, Alosa DM, Renstrom AF, Trevino S, Beynnon B. A prospective study of ankle injury risk factors. Am J Sports Med. 1995;23(5):564–570. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
