

Prehypertension and incidence of cardiovascular disease: a meta-analysis
- PMID: 23915102
- PMCID: PMC3750349
- DOI: 10.1186/1741-7015-11-177
Prehypertension and incidence of cardiovascular disease: a meta-analysis
Abstract
Background: Prospective cohort studies of prehypertension and the incidence of cardiovascular disease (CVD) are controversial after adjusting for other cardiovascular risk factors. This meta-analysis evaluated the association between prehypertension and CVD morbidity.
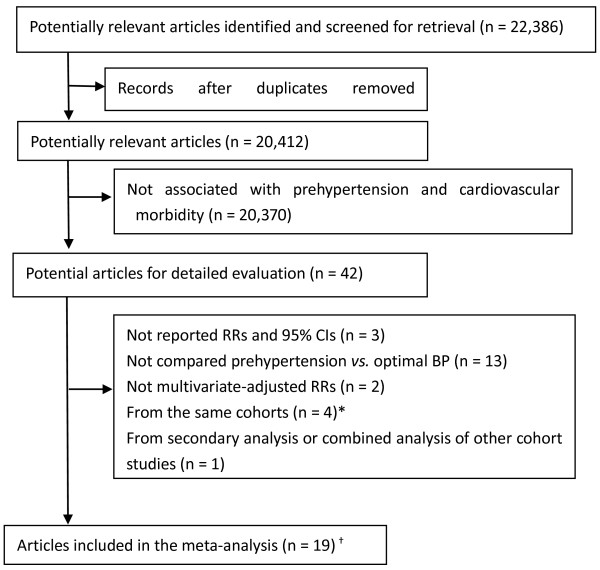
Methods: Databases (PubMed, EMBASE and the Cochrane Library) and conference proceedings were searched for prospective cohort studies with data on prehypertension and cardiovascular morbidity. Two independent reviewers assessed the reports and extracted data. The relative risks (RRs) of CVD, coronary heart disease (CHD) and stroke morbidity were calculated and reported with 95% confidence intervals (95% CIs). Subgroup analyses were conducted on blood pressure, age, gender, ethnicity, follow-up duration, number of participants and study quality.
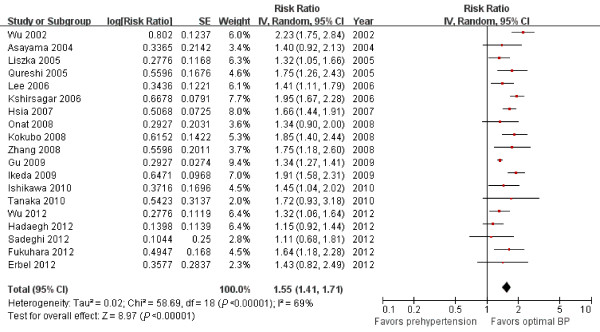
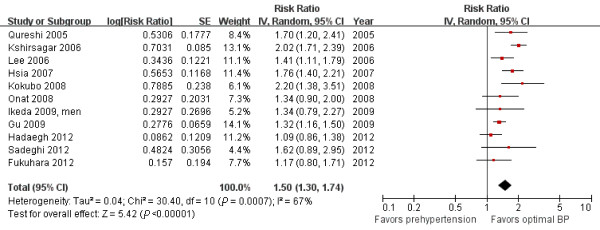
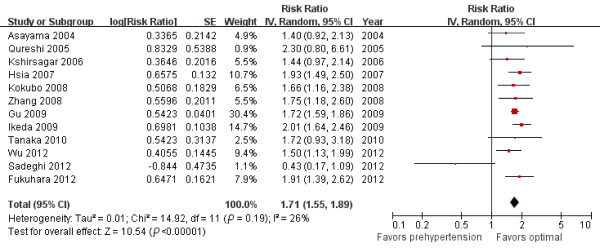
Results: Pooled data included the results from 468,561 participants from 18 prospective cohort studies. Prehypertension elevated the risks of CVD (RR = 1.55; 95% CI = 1.41 to 1.71); CHD (RR = 1.50; 95% CI = 1.30 to 1.74); and stroke (RR = 1.71; 95% CI = 1.55 to 1.89). In the subgroup analyses, even for low-range prehypertension, the risk of CVD was significantly higher than for optimal BP (RR = 1.46, 95% CI = 1.32 to 1.62), and further increased with high-range prehypertension (RR = 1.80, 95% CI = 1.41 to 2.31). The relative risk was significantly higher in the high-range prehypertensive populations than in the low-range populations (χ2= 5.69, P = 0.02). There were no significant differences among the other subgroup analyses (P>0.05).
Conclusions: Prehypertension, even in the low range, elevates the risk of CVD after adjusting for multiple cardiovascular risk factors.
Figures
Comment in
-
Pre-hypertension: another 'pseudodisease'?BMC Med. 2013 Sep 25;11:211. doi: 10.1186/1741-7015-11-211. BMC Med. 2013. PMID: 24229371 Free PMC article.
References
-
- Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JJ, Jones DW, Materson BJ, Oparil S, Wright JT Jr, Roccella EJ. National Heart, Lung, and Blood Institute Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; National High Blood Pressure Education Program Coordinating Committee. The seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure: the JNC 7 report. JAMA. 2003;289:2560–2572. doi: 10.1001/jama.289.19.2560. Erratum in: JAMA 2003, 290:197. - DOI - PubMed
-
- Lewington S, Clarke R, Qizilbash N, Peto R, Collins R. Prospective Studies Collaboration. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360:1903–1913. Erratum in: Lancet 2003, 361:1060. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
