

Interdisciplinary decision making in prostate cancer therapy - 5-years' time trends at the Interdisciplinary Prostate Cancer Center (IPC) of the Charité Berlin
- PMID: 23915212
- PMCID: PMC3751298
- DOI: 10.1186/1472-6947-13-83
Interdisciplinary decision making in prostate cancer therapy - 5-years' time trends at the Interdisciplinary Prostate Cancer Center (IPC) of the Charité Berlin
Abstract
Background: Patients with prostate cancer face the difficult decision between a wide range of therapeutic options. These men require elaborate information about their individual risk profile and the therapeutic strategies´ risks and benefits to choose the best possible option. In order to detect time trends and quality improvements between an early patient population (2003/2004) and a later reference group (2007/2008) data was analysed with regards to epidemiologic parameters, differences in diagnostics and the type and ranking of the recommended therapies taking into account changes to Gleason Grading System and implementation of new therapeutic strategies, particularly Active surveillance, in 2005.
Methods: Data from all 496 consecutive patients who received consultation in 2003/2004 (n = 280) and 2007/2008 (n = 216) was retrospectively evaluated. Categorical variables were compared using the Chi-square test. Dependent variables were analysed using the unpaired Students´ t-test and the Mann-Whitney U-test.
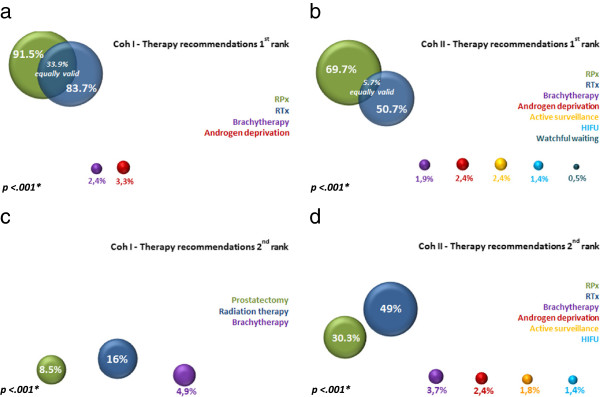
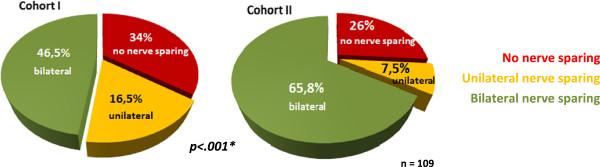
Results: The cohorts were comparable concerning clinical stage, initial PSA, prostate volume, comorbidities and organ confined disease. Patients in Cohort I were younger (66.44 vs. 69.31y; p < .001) and had a longer life expectancy (17.22 vs. 14.75y; p < .001). 50.9%, 28.2% and 20.9% in Cohort I and 37.2%, 39.6% and 23.2% in Cohort II showed low-, intermediate- and high-risk disease (D´Amico) with a trend towards an increased risk profile in Cohort II (p = .066). The risk-adapted therapy recommended as first option was radical prostatectomy for 91.5% in Cohort I and 69.7% in Cohort II, radiation therapy for 83.7% in Cohort I and 50.7% in Cohort II, and other therapies (brachytherapy, Active surveillance, Watchful waiting, high-intensity focused ultrasound) for 6.5% in Cohort I and 6.9% in Cohort II (p < .001). Radiation therapy was predominant in both cohorts as second treatment option (p < .001). Time trends showing quality improvement involved an increase in biopsy cores (9.95 ± 2.38 vs. 8.43 ± 2.29; p < .001) and an increased recommendation for bilateral nerve sparing (p < .001).
Conclusion: In the earlier years, younger patients with a more favourable risk profile presented for interdisciplinary consultation. A unilateral recommendation for radical prostatectomy and radiation therapy was predominant. In the later years, the patient population was considerably older. However, this group may have benefitted from optimised diagnostic possibilities and a wider range of treatment options.
Figures
References
-
- GEKID. Cancer in Germany 2007/2008, Version 8. Berlin, Germany: Robert-Koch-Institute and the Association of Population-based Cancer Registries in Germany (GEKID); 2012.
-
- Macintosh CA, Stower M, Reid N, Maitland NJ. Precise microdissection of human prostate cancers reveals genotypic heterogeneity. Cancer Res. 1998;58(1):23–28. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
