

Diagnosing delirium in older emergency department patients: validity and reliability of the delirium triage screen and the brief confusion assessment method
- PMID: 23916018
- PMCID: PMC3936572
- DOI: 10.1016/j.annemergmed.2013.05.003
Diagnosing delirium in older emergency department patients: validity and reliability of the delirium triage screen and the brief confusion assessment method
Abstract
Study objective: Delirium is a common form of acute brain dysfunction with prognostic significance. Health care professionals caring for older emergency department (ED) patients miss delirium in approximately 75% of cases. This error results from a lack of available measures that can be performed rapidly enough to be incorporated into clinical practice. Therefore, we developed and evaluated a novel 2-step approach to delirium surveillance for the ED.
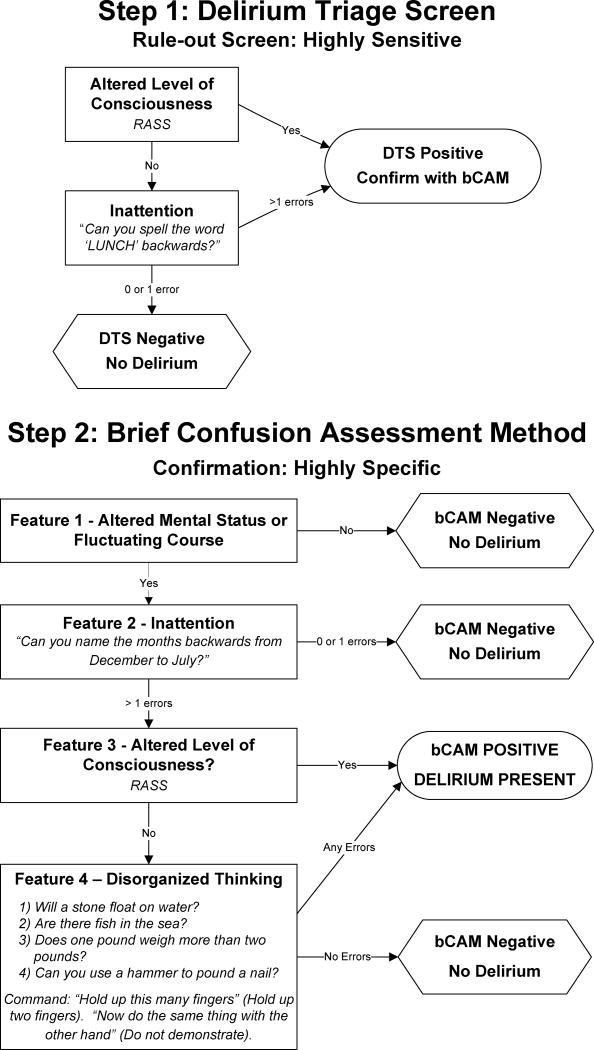
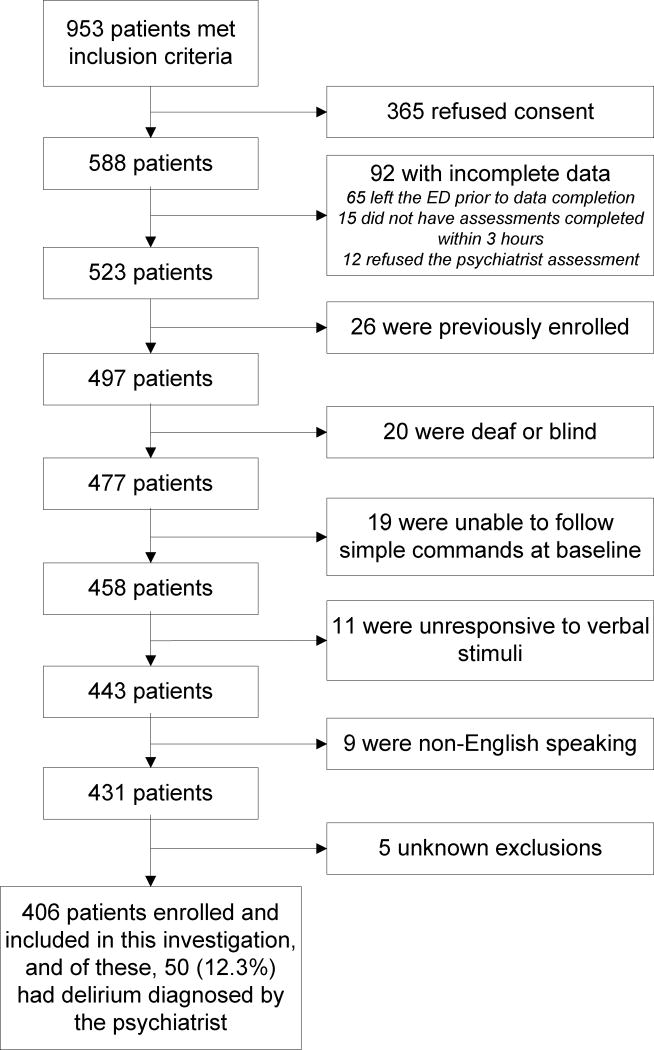
Methods: This prospective observational study was conducted at an academic ED in patients aged 65 years or older. A research assistant and physician performed the Delirium Triage Screen (DTS), designed to be a highly sensitive rule-out test, and the Brief Confusion Assessment Method (bCAM), designed to be a highly specific rule-in test for delirium. The reference standard for delirium was a comprehensive psychiatrist assessment using Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision criteria. All assessments were independently conducted within 3 hours of one another. Sensitivities, specificities, and likelihood ratios with their 95% confidence intervals (95% CIs) were calculated.
Results: Of 406 enrolled patients, 50 (12.3%) had delirium diagnosed by the psychiatrist reference standard. The DTS was 98.0% sensitive (95% CI 89.5% to 99.5%), with an expected specificity of approximately 55% for both raters. The DTS's negative likelihood ratio was 0.04 (95% CI 0.01 to 0.25) for both raters. As the complement, the bCAM had a specificity of 95.8% (95% CI 93.2% to 97.4%) and 96.9% (95% CI 94.6% to 98.3%) and a sensitivity of 84.0% (95% CI 71.5% to 91.7%) and 78.0% (95% CI 64.8% to 87.2%) when performed by the physician and research assistant, respectively. The positive likelihood ratios for the bCAM were 19.9 (95% CI 12.0 to 33.2) and 25.2 (95% CI 13.9 to 46.0), respectively. If the research assistant DTS was followed by the physician bCAM, the sensitivity of this combination was 84.0% (95% CI 71.5% to 91.7%) and specificity was 95.8% (95% CI 93.2% to 97.4%). If the research assistant performed both the DTS and bCAM, this combination was 78.0% sensitive (95% CI 64.8% to 87.2%) and 97.2% specific (95% CI 94.9% to 98.5%). If the physician performed both the DTS and bCAM, this combination was 82.0% sensitive (95% CI 69.2% to 90.2%) and 95.8% specific (95% CI 93.2% to 97.4%).
Conclusion: In older ED patients, this 2-step approach (highly sensitive DTS followed by highly specific bCAM) may enable health care professionals, regardless of clinical background, to efficiently screen for delirium. Larger, multicenter trials are needed to confirm these findings and to determine the effect of these assessments on delirium recognition in the ED.
Copyright © 2013 American College of Emergency Physicians. Published by Mosby, Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Blazer DG, van Nieuwenhuizen AO. Evidence for the diagnostic criteria of delirium: an update. Curr Opin Psychiatry. 2012;25:239–243. - PubMed
-
- Hustey FM, Meldon SW, Smith MD, et al. The effect of mental status screening on the care of elderly emergency department patients. Ann Emerg Med. 2003;41:678–684. - PubMed
-
- Niska R, Bhuiya F, Xu J. National Hospital Ambulatory Medical Care Survey: 2007 emergency department summary. Natl Health Stat Report. 2010:1–31. - PubMed
Publication types
MeSH terms
Grants and funding
- UL1 TR000445/TR/NCATS NIH HHS/United States
- K23AG032355/AG/NIA NIH HHS/United States
- R01 AG035117/AG/NIA NIH HHS/United States
- K12 HL109019/HL/NHLBI NIH HHS/United States
- R01AG027472/AG/NIA NIH HHS/United States
- R01 AG027472/AG/NIA NIH HHS/United States
- UL1 RR024975/RR/NCRR NIH HHS/United States
- K23 AG032355/AG/NIA NIH HHS/United States
- UL1 RR024975-01/RR/NCRR NIH HHS/United States
- 2 UL1 TR000445-06/TR/NCATS NIH HHS/United States
- R01AG035117/AG/NIA NIH HHS/United States
- K23 AG040157/AG/NIA NIH HHS/United States
- K23AG040157/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
