

Pediatric neuroimaging using magnetic resonance imaging during non-sedated sleep
- PMID: 23917588
- PMCID: PMC3889986
- DOI: 10.1007/s00247-013-2752-8
Pediatric neuroimaging using magnetic resonance imaging during non-sedated sleep
Abstract
Background: Etiological studies of many neurological and psychiatric disorders are increasingly turning toward longitudinal investigations of infant brain development in order to discern predisposing structural and/or functional differences prior to the onset of overt clinical symptoms. While MRI provides a noninvasive window into the developing brain, MRI of infants and toddlers is challenging due to the modality's extreme motion sensitivity and children's difficulty in remaining still during image acquisition.
Objective: Here, we outline a broad research protocol for successful MRI of children under 4 years of age during natural, non-sedated sleep.
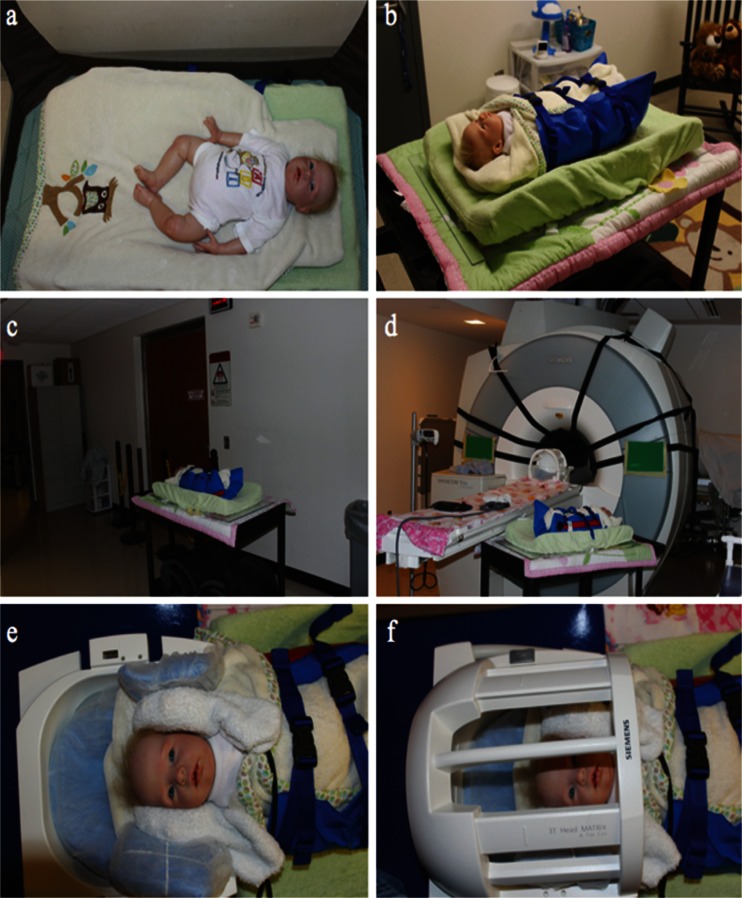
Materials and methods: All children were imaged during natural, non-sedated sleep. Active and passive measures to reduce acoustic noise were implemented to reduce the likelihood of the children waking up during acquisition. Foam cushions and vacuum immobilizers were used to limit intra-scan motion artifacts.
Results: More than 380 MRI datasets have been successfully acquired from 220 children younger than 4 years of age within the past 39 months. Implemented measures permitted children to remain asleep for the duration of the scan and allowed the data to be acquired with an overall 97% success rate.
Conclusion: The proposed method greatly advances current pediatric imaging techniques and may be readily implemented in other research and clinical settings to facilitate and further improve pediatric neuroimaging.
Figures





References
-
- Woods-Frohlich L, Martin T. Training children to reduce motion and increase success of MRI scanning. Curr Med Imaging Rev. 2010;6:165–170. doi: 10.2174/157340510791636255. - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
