

Advances in MR imaging for cervical spondylotic myelopathy
- PMID: 23917647
- PMCID: PMC4879123
- DOI: 10.1007/s00586-013-2915-1
Advances in MR imaging for cervical spondylotic myelopathy
Abstract
Purpose: To outline the pathogenesis of cervical spondylotic myelopathy (CSM), the correlative abnormalities observed on standard magnetic resonance imaging (MRI), the biological implications and current status of diffusion tensor imaging (DTI), and MR spectroscopy (MRS) as clinical tools, and future directions of MR technology in the management of CSM patients.
Methods: A systematic review of the pathogenesis and current state-of-the-art in MR imaging technology for CSM was performed.
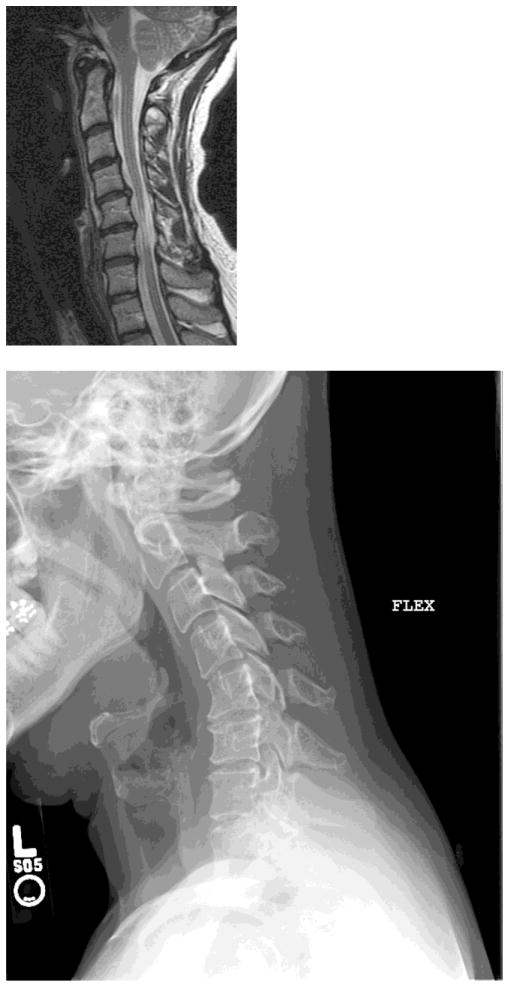
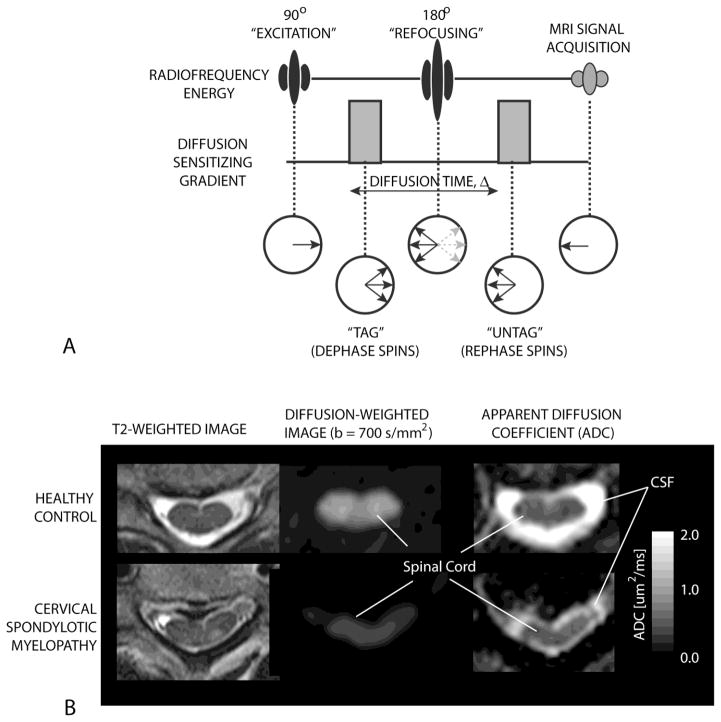
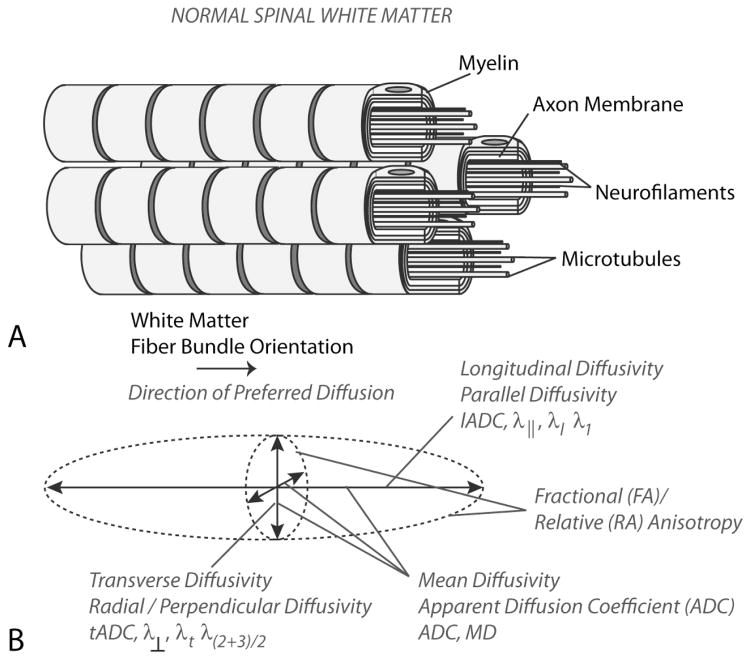
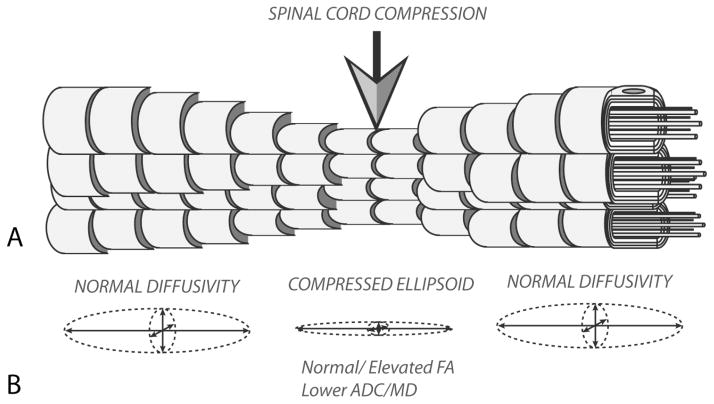
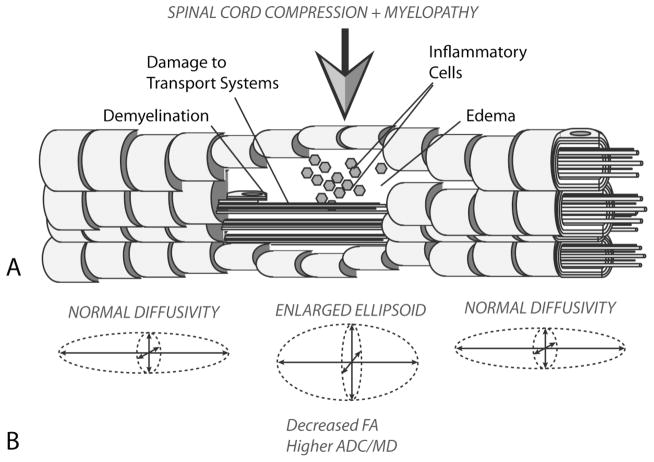
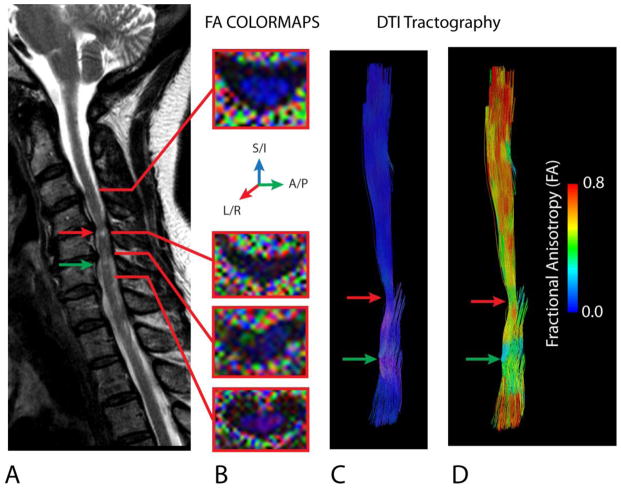
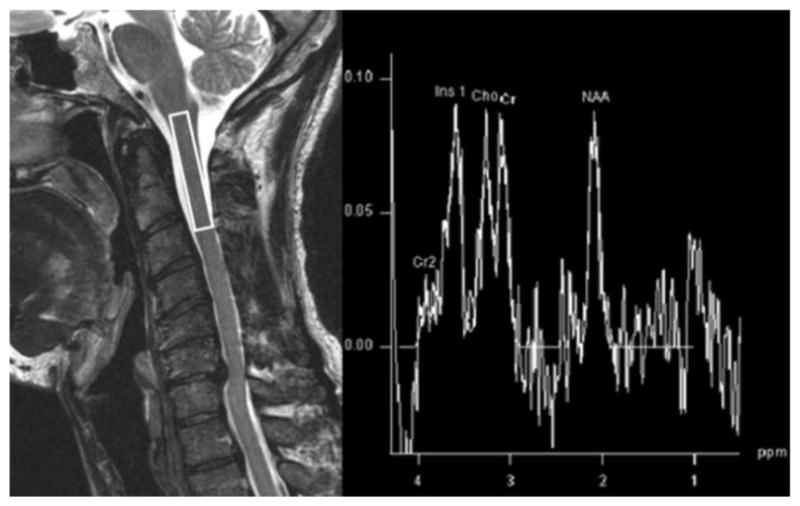
Results: CSM is caused by progressive, degenerative, vertebral column abnormalities that result in spinal cord damage related to both primary mechanical and secondary biological injuries. The T2 signal change on conventional MRI is most commonly associated with neurological deficits, but tends not to be a sensitive predictor of recovery of function. DTI and MRS show altered microstructure and biochemistry that reflect patient-specific pathogenesis.
Conclusion: Advanced imaging techniques, including DTI and MRS, show higher sensitivity to microstructural and biochemical changes within the cord, and may aid in management of CSM patients.
Figures

References
-
- Demir A, Ries M, Moonen CT, Vital JM, Dehais J, Arne P, Caille JM, Dousset V. Diffusion-weighted MR imaging with apparent diffusion coefficient and apparent diffusion tensor maps in cervical spondylotic myelopathy. Radiology. 2003;229:37–43. - PubMed
-
- Hernandez E, Mackay AL, MacMillan EL, Madler B, Li DK, Dvorak MF, Cordova T, Ramirez-Manzanares A, Laule C. Diffusion tensor imaging of subjects with Cervical Spondylotic Myelopathy: use of the eigenvalues as indicators of spinal stenosis. Proc Intl Soc Mag Reson Med. 2009;17:1309.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
