

Risk factors and classifications of hilar cholangiocarcinoma
- PMID: 23919107
- PMCID: PMC3731526
- DOI: 10.4251/wjgo.v5.i7.132
Risk factors and classifications of hilar cholangiocarcinoma
Abstract
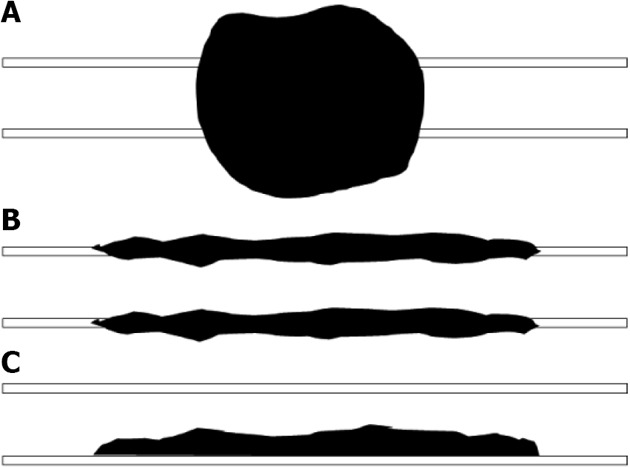
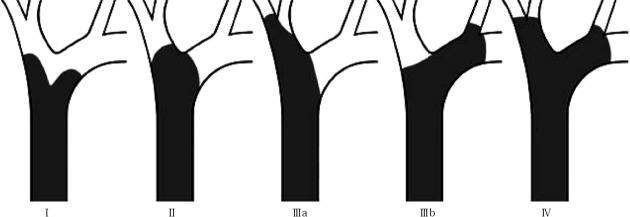
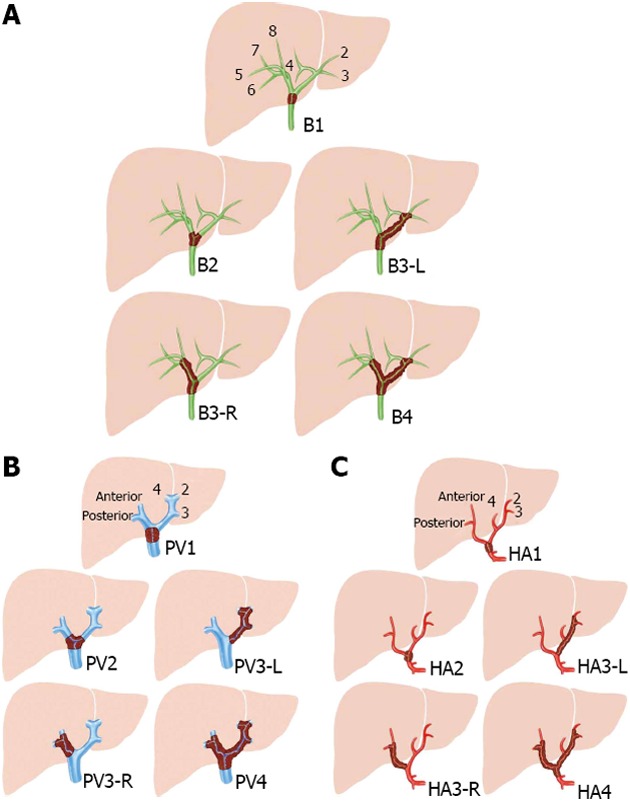
Cholangiocarcinoma is the second most common primary malignant tumor of the liver. Perihilar cholangiocarcinoma or Klatskin tumor represents more than 50% of all biliary tract cholangiocarcinomas. A wide range of risk factors have been identified among patients with Perihilar cholangiocarcinoma including advanced age, male gender, primary sclerosing cholangitis, choledochal cysts, cholelithiasis, cholecystitis, parasitic infection (Opisthorchis viverrini and Clonorchis sinensis), inflammatory bowel disease, alcoholic cirrhosis, nonalcoholic cirrhosis, chronic pancreatitis and metabolic syndrome. Various classifications have been used to describe the pathologic and radiologic appearance of cholangiocarcinoma. The three systems most commonly used to evaluate Perihilar cholangiocarcinoma are the Bismuth-Corlette (BC) system, the Memorial Sloan-Kettering Cancer Center and the TNM classification. The BC classification provides preoperative assessment of local spread. The Memorial Sloan-Kettering cancer center proposes a staging system according to three factors related to local tumor extent: the location and extent of bile duct involvement, the presence or absence of portal venous invasion, and the presence or absence of hepatic lobar atrophy. The TNM classification, besides the usual descriptors, tumor, node and metastases, provides additional information concerning the possibility for the residual tumor (R) and the histological grade (G). Recently, in 2011, a new consensus classification for the Perihilar cholangiocarcinoma had been published. The consensus was organised by the European Hepato-Pancreato-Biliary Association which identified the need for a new staging system for this type of tumors. The classification includes information concerning biliary or vascular (portal or arterial) involvement, lymph node status or metastases, but also other essential aspects related to the surgical risk, such as remnant hepatic volume or the possibility of underlying disease.
Keywords: Bile duct cancer; Hilar cholangiocarcinoma; Klatskin tumor; Perihilar cholangiocarcinoma.
Figures
References
-
- Jarnagin WR, Shoup M. Surgical management of cholangiocarcinoma. Semin Liver Dis. 2004;24:189–199. - PubMed
-
- Friman S. Cholangiocarcinoma--current treatment options. Scand J Surg. 2011;100:30–34. - PubMed
-
- Shin HR, Oh JK, Masuyer E, Curado MP, Bouvard V, Fang Y, Wiangnon S, Sripa B, Hong ST. Comparison of incidence of intrahepatic and extrahepatic cholangiocarcinoma--focus on East and South-Eastern Asia. Asian Pac J Cancer Prev. 2010;11:1159–1166. - PubMed
-
- Khan SA, Emadossadaty S, Ladep NG, Thomas HC, Elliott P, Taylor-Robinson SD, Toledano MB. Rising trends in cholangiocarcinoma: is the ICD classification system misleading us? J Hepatol. 2012;56:848–854. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
