

Refining angiographic biomarkers of revascularization: improving outcome prediction after intra-arterial therapy
- PMID: 23920017
- PMCID: PMC4142767
- DOI: 10.1161/STROKEAHA.113.001990
Refining angiographic biomarkers of revascularization: improving outcome prediction after intra-arterial therapy
Abstract
Background and purpose: Angiographic revascularization grading after intra-arterial stroke therapy is limited by poor standardization, making it unclear which scale is optimal for predicting outcome. Using recently standardized criteria, we sought to compare the prognostic performance of 2 commonly used reperfusion scales.
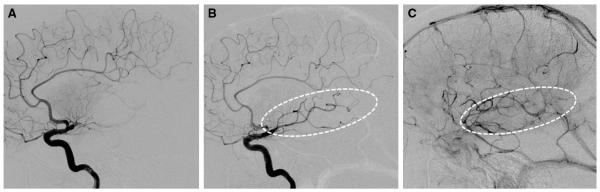
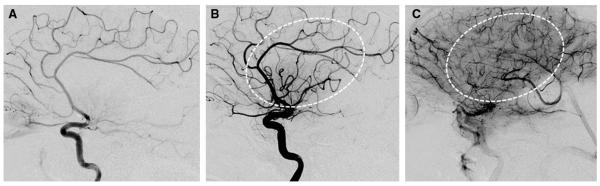
Methods: Inclusion criteria for this multicenter retrospective study were acute ischemic stroke attributable to middle cerebral artery M1 occlusion, intra-arterial therapy, and 90-day modified Rankin scale score. Post-intra-arterial therapy reperfusion was graded using the Thrombolysis in Myocardial Infarction (TIMI) and Modified Thrombolysis in Cerebral Infarction (mTICI) scales. The scales were compared for prediction of clinical outcome using receiver-operating characteristic analysis.
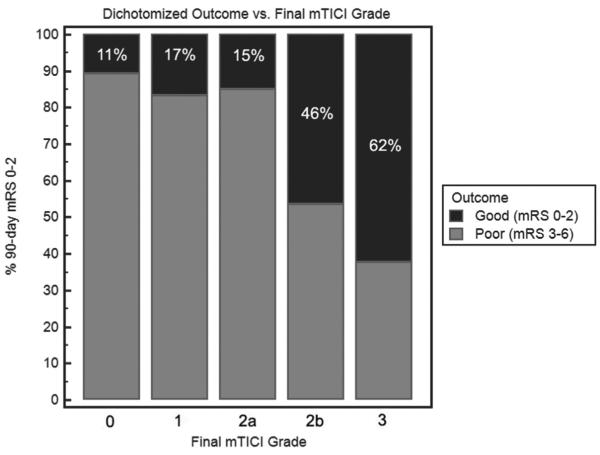
Results: Of 308 patients, mean age was 65 years, and median National Institutes of Health Stroke Scale score was 17. The mean time from stroke onset to groin puncture was 305 minutes. There was no difference in the time to treatment between patients grouped by final TIMI (ie, 0 versus 1 versus 2 versus 3) or mTICI grades (ie, 0 versus 1 versus 2a versus 2b versus 3). Good outcome (modified Rankin scale, 0-2) was achieved in 32.5% of patients, and mortality rate was 25.3% at 90 days. There was a 6.3% rate of parenchymal hematoma type 2. In receiver-operating characteristic analysis, mTICI was superior to TIMI for predicting 90-day modified Rankin scale 0 to 2 (c-statistic: 0.74 versus 0.68; P<0.0001). The optimal threshold for identifying a good outcome was mTICI 2b to 3 (sensitivity 78.0%; specificity 66.1%).
Conclusions: mTICI is superior to TIMI for predicting clinical outcome after intra-arterial therapy. mTICI 2b to 3 is the optimal biomarker for procedural success.
Keywords: TIMI; acute ischemic stroke; endovascular; intra-arterial therapy; modified TICI; revascularization.
Figures
References
-
- Rha JH, Saver JL. The impact of recanalization on ischemic stroke outcome: a meta-analysis. Stroke. 2007;38:967–973. - PubMed
-
- Penumbra Pivotal Stroke Trial Investigators The penumbra pivotal stroke trial: safety and effectiveness of a new generation of mechanical devices for clot removal in intracranial large vessel occlusive disease. Stroke. 2009;40:2761–2768. - PubMed
-
- Saver JL, Jahan R, Levy EI, Jovin TG, Baxter B, Nogueira RG, et al. SWIFT Trialists Solitaire flow restoration device versus the Merci Retriever in patients with acute ischaemic stroke (SWIFT): a randomised, parallel-group, non-inferiority trial. Lancet. 2012;380:1241–1249. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
